

From the Sunday Age:

Illustration: Matt Davidson.
One of the outstanding developments in medical care in the past 40 years has been palliative care. Yet it would be more widely embraced if in its practice it better respected people's choices and offered them the option of when to die if their needs could not be met.
Palliative care was established in the early 1970s due to the work of Dame Cicely Saunders in Britain. It is now widely supported by governments and is central to end-of-life policy in Victoria.
It was initiated by people with strong Christian belief; and the early hospices were run by religious institutions. Religion has played a central part in its development; today the Catholic Church provides nearly 60 per cent of palliative care in Australia. There is no other area of medical care in Australia where a religious group has such dominance in provision of care.
The World Health Organisation states that "palliative care provides relief from pain and other distressing symptoms, affirms life and regards dying as a normal process and intends neither to hasten nor to prolong death" – an ambitious philosophy.
Missionary surgeon and later esteemed palliative care specialist Derek Doyle wrote that "a metaphorical halo shines over specialist palliative care and its practitioners with the result that some of its claims and assumptions have gone unchallenged by all but a few". Social anthropologist Julia Lawton was one who has challenged this view. She embedded herself in palliative care for 10 months – she found it did not match its rhetoric.
Palliative care consultant Fiona Randall was another critic – she drew attention to "the inflated and often contradictory claims made in the literature of palliative care".
"Palliative medicine claims to alleviate emotional, psychological, social and spiritual suffering, in addition to physical symptoms,'' she said. "There is no other specialty that claims to do all these. Moreover, palliative medicine claims to be able to alleviate these forms of distress and improve quality of life, even in the context of dying. Dying is generally perceived to be associated with great distress, yet in palliative care it is held that we can still achieve relief of symptoms, including those of psychosocial and spiritual nature."
Palliative care states that it offers 'impeccable' assessment and treatment of pain, and that nursing care is "exquisite" and "meticulous". Randall describes this as "embarrassing rhetoric". Palliative care does lay great emphasis on its ability to relieve pain, yet Professor Michael Cousins, Australia's foremost pain specialist, stated in 2010 that "10 per cent of cancer pain was so difficult to treat at the end of their life" that some patients were given drugs to sedate them to unconsciousness, culminating in death over several days to a week.
Palliative care makes every effort to improve its outcomes – there are over 20 journals devoted to reporting on the treatment and outcomes, but almost all of this information remains 'in house' and the public are blissfully unaware of the reality. Occasional attempts have been made to assess the efficacy of palliative care.
In 2008, Camilla Zimmermann and colleagues analysed the PC literature and found that "only one trial demonstrated benefit from the palliative care intervention for any of the individual symptoms measured", and "there is scant evidence to support the effectiveness of specialised care for patients with terminal illness in terms of quality of life, patient and care giver satisfaction or economic cost". The earlier study of Salisbury also found "there is little robust evidence that any form of organisation of specialised palliative care offers significant advantages in terms of impact on patients' quality of life".
These are harsh judgments because the progressive nature of dying makes scientific study of intervention extremely difficult – one is always trying to catch up with escalating symptoms; nevertheless, it is important to note that while there is much anecdotal evidence of the value of palliative care, there is a dearth of scientific support.
Given the extraordinarily difficult task palliative care sets itself, it would not be surprising to find that some people request hastening of death in palliative care. A study by Adelaide palliative care specialist Roger Hunt and colleagues found 25 per cent of their terminal patients wanted a hastened death, and other eminent researchers into dying found very similar results.
So what does palliative care do for people who request assistance to die. The position statement of American Academy of Hospice and Palliative Medicine indicates that if the request cannot be deflected, the patient should be offered "a discontinuation of life-prolonging treatment" (not all patients have such an option); or "voluntary cessation of eating and drinking"; or "palliative sedation, even potentially to unconsciousness". Because palliative care does not hasten death, this latter option is employed gradually, by titration of medication, such that when the initial dose does not relieve suffering, an increase of dose is justified, and so on, until eventually complete control of symptoms is achieved, usually by unconsciousness, followed by death. Just where in this process the family can say goodbye is a mystery.
Many people cannot see why it is so important to go to the very end of the line, which is at the core of the palliative care philosophy. Many might say I would like to go as the sun is setting and not go on into the darkness.
What logic is there in demanding that an unhastened death by dehydration or drug-induced coma is all that can be offered. To return to Randall – "the goal [of impeccable relief of pain and other symptoms] is unachievable and the expectations generated by the philosophy of palliative care are unrealistic. Setting unachievable goals for one set of people, and promoting unrealistic expectations (which will not be met) in another group of people, is unfair to both and likely to lead to harm for both."
Let me conclude with the opinion of a Professor of Palliative Medicine, Sam Ahmedzai, from Sheffield, expressed in the British medical Journal in 2012. "It is patronising to say that a few people should suffer unbearable distress and indignity because palliative care preaches that it values all lives – regardless of how meaningless they have become to their owners. It is inconsistent for palliative care to boast how it enables people to face the reality of dying and decide about the place of care but then to deny choice for timing of death. Moreover, it is hypocritical to deny competent patients who are acknowledged to be dying the right to die in the manner of their choosing, while allowing doctors and nurses to choose when to place them on a care pathway, which often entails increasing sedation and withdrawing fluids – unintentionally leading to a protracted form of assisted dying, but one that is medically determined."
The evidence does not support governments repeating that palliative care resolves the need for the development of unambiguous end of life legislation.
Dr Rodney Syme is a voluntary euthanasia campaigner.
From The Age:
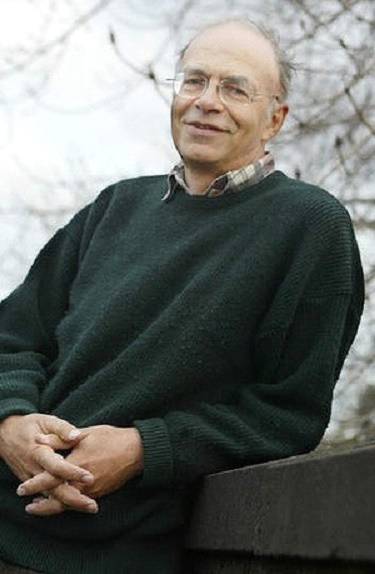
Professor of Ethics Peter Singer. Photo: Joe Armao
Ethicist Peter Singer has questioned the Medical Board of Australia’s decision to suspend euthanasia campaigner Philip Nitschke’s medical registration, and says the only way to protect vulnerable people from him is to legalise voluntary euthanasia.
In an interview with Fairfax Media, the professor of bioethics at Princeton University said it would be both ‘‘concerning’’ and ‘‘extraordinary’’ if the medical board had suspended Dr Nitschke because he believed people without a terminal illness could make a rational decision to die.
‘‘I think suicide can be rational in the absence of terminal illness and I think I could find you dozens or hundreds of philosophers who would think that ... I think if you know you are going to spend the next 20 years in prison, suicide is a rational option - not for everybody, but for some people,’’ he said, referring to the case of Nigel Brayley, a Perth man who communicated with Dr Nitschke before taking his own life while he was being investigated over his wife's death.
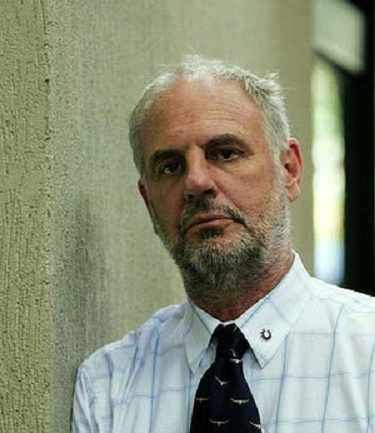
Euthanasia campaigner Dr Philip Nitschke. Photo: Ryan Osland
In July, Dr Nitschke said the board suspended his registration because his view that ‘‘people have a right to choose suicide is incompatible with his responsibility as a doctor” and because he posed “a serious risk to public health and safety that needs to be managed”.
This followed media reports that Mr Brayley, 45, was suspected to be suffering depression, had attended an Exit International workshop in February ,and communicated with Dr Nitschke before he took his own life in May.
Dr Nitschke has confirmed that Mr Brayley attended an Exit workshop, but said he had not lost his capacity to make a rational decision. He said he did not give Mr Brayley medical advice and had no obligation to refer him to a psychiatrist. He said Mr Brayley was a "wife killer" and that his death was "a clear case of rational suicide".
Dr Nitschke has appealed the board’s ‘‘political’’ decision and says those who claimed Mr Brayley was depressed were fundamentalist Christians.
The case has intensified criticism of Dr Nitschke, with several Australian parents claiming their adult children took their own lives after accessing Exit International information. The Australian Medical Association, beyondblue and Dying with Dignity have all since questioned his actions, too, with some accusing him of being irresponsible.
The Medical Board of Australia has not detailed its reasons for suspending Dr Nitschke’s registration, except to say it is trying to ‘‘keep the public safe, while other investigations or processes continue’’.
Professor Singer said it would be strange for the board to make ‘‘a moral judgment and by no means a universally accepted moral judgment’’ about rational suicide.
‘‘Using that as a grounds for suspending a doctor’s medical licence, I think is very strange,’’ he said.
In response to concerns about depressed people accessing Exit International information, Professor Singer said: ‘‘I think the solution to that is to legalise voluntary euthanasia and restrict it to medical practitioners, and then Philip won’t have to do this ... I think he feels he is a crusader against a law that unnecessarily restricts people's right to die.''
Professor Singer, who was in Australia to attend the Queensland University of Technology’s International Conference on End of Life last week, said he believed the legalisation of voluntary euthanasia or assisted suicide was inevitable in Australia. ‘‘I think it will come as the population ages ... I think we'll get voting pressure for it,’’ he said.
For help or information call Suicide Helpline Victoria on 1300 651 251 or Lifeline on 131 114, or visit beyondblue.org.au.
In the 1990s when people were dying with AIDS-related diseases in great agony and distress, many people who were caring for them - doctors, nurses, carers, partners, friends, family, assisted their dying processes. I do not have evidence but this is believed to continue to this day in August 2014 without anyone commenting or making others aware of it.
Voluntary euthanasia needs to be legalised,
Our pets are euthanased when their pain becomes unbearable.
We need to be legally entitled to euthanasia too.
Letters in The Age:
The palliative care argument has one primary flaw that is often overlooked. It is not, and cannot be, a successful option in all cases. Even if palliation is 99 per cent successful, we cannot ignore the remaining 1 per cent as if those people don't matter. Society, and therefore governments, should not try to rationalise that residual, relentless suffering simply because it represents a minority of dying individuals. Do their deaths simply fall under the heading of ''collateral damage''? I hope not. It is suggested we need an ''open discussion about the ethics, moral imperatives and potential pitfalls'', as though this will lead to the government acting upon communal expectations. Here is the reality. That conversation has already happened many, many times over many, many years. The government already knows what the community wants. All that is lacking, which has been for those years, is the will, the compassion and the political backbone for the government to listen to that conversation. This government already has a mandate to introducing assisted dying laws. Apparently not all ''mandates'' are equal.
Bob Thomas, Blackburn SouthPaul Cocks (Letters, 24/8) insists that the choice of a suffering dying person should be denied to uphold the ''absolute'' values of civilisation; or, as 80 per cent of Australians support dying with dignity and 5 per cent are undecided, he means the absolutist values of 15 per cent of the population. He should be free to suffer this way if he wants, but he doesn't explain why intolerable suffering at the end is better than not suffering; nor why his views on suffering should be forced on others.
Janine Truter, The BasinI don't think I will ever come to terms with my dear mum's ordeal in palliative care. Mum was a gentle soul who spent most of her adult life unselfishly caring for other people, while also maintaining a home and family. She suffered from dementia in later life, but other medical issues intervened that brought forward the inevitable. Mum was in an aged care facility that also provided palliative care. My experience was that while there were many caring staff members, there were inconsistent views on palliative care procedures depending on who was in charge. Some enforced their beliefs, but most were in fear of not being seen to assist a resident pass away, even to the point of withholding pain relief. Thus my mum's life ended in an undignified, painful and drawn-out manner. Even on the day she passed away we had to go over the head of the nurse in charge to have pain relief administered.
Nobody deserves to have their life end in such an inhumane and undignified manner.There is a need in palliative care for legally assisted euthanasia to put an end to these drawn-out processes with inevitable outcomes. Palliative care patients should be cared for in separate specialised facilities, with compassionate staff who have clear guidelines in how to handle this vulnerable time for patients and their families. Until someone overhauls the system, sad stories from families in despair will continue to appear.
Name and address withheldFrom The Age:

Simon Benson has strong views on assisted death. Photo: Angela Wylie
The man was obviously emotional, recalls Simon Benson. But he did not cry. Instead he asked what was possibly the hardest question of his life: How can I help my mother die?
Benson was not all that surprised. The affable Footscray GP had treated the woman and her son for years and she had already told him she had no intention of being kept alive through the final stages of glioblastoma – a frightening cancer that can distort one's personality in distressing ways.
The woman was in her 80s. She had lived an independent life, and wanted the same sort of death. She had already told Benson that she did not want to reach a point where she could not look after herself. Her son was now living interstate. She wanted him to do this one last thing for her.
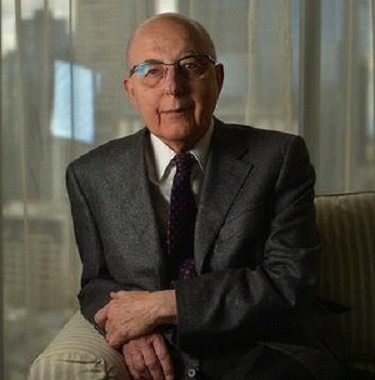
Retired cardiologist Peter Valentine. Photo: Michael Clayton-Jones
"I told him to give her a big dose of morphine[and another drug] she had while she was in palliative care and to put a plastic bag over her head,"Benson says. "He said, 'If that's what I have to do, that's what I have to do'."
Taking lives, rather than saving them, is not something many doctors aspire to. But the old adage "first do no harm" has been challenged in recent years by euthanasia campaigners Rodney Syme and Philip Nitschke who say they have both helped countless people die when they thought it was the most compassionate thing to do.
It is unclear how many doctors make similar decisions each year. In 2007, a survey of 854 Victorian doctors found that 302 had been asked at least once to hasten someone's death by giving them drugs. Of that number, about a third said they had agreed.
While few doctors have spoken publicly about such cases, three Melbourne doctors have decided to reveal their experiences in The Sunday Age because they believe physician-assisted death should be legalised. In Victoria, euthanasia and assisted suicide are both illegal, carrying penalties of up to 25 years' jail. So far, no politicians have announced any plans to examine legalisation ahead of this year's state election.
Another doctor. Another mother. Before he retired, Peter Valentine was a cardiologist. He looked after people's hearts. But this did not help much when it came to caring for his own mother in her final years as she endured the severe pain and immobility of rheumatoid arthritis. That task fell to her GP.
Valentine says that when she became too weak to walk and feared being unable to remain in her home, the 81-year-old told her GP that she did not want to go on. Valentine believes that what happened next was not an accident. The GP gave her a cache of strong sedatives and advised her that a certain number of tablets would be "a very dangerous dose," Valentine says. "So I'm certain he knew."
About three months later, Mrs Valentine asked her son to be with her in her Hawthorn home. The two had spoken on several occasions about her wish to die. Valentine was convinced she was sane and rational. She was not depressed. Her condition was incurable. And she was only going to get worse.
"She took her life with my help in the sense that I was present and I handed her the tablets," he says.
She breathed for about five more minutes, Valentine says. And then she stopped.
"I held her as she died ... and I knew it was an infinitely better death than the one staring her in the face," he says.
Later, he called his mother's doctor to come and confirm the death. The death certificate the doctor wrote listed her various medical conditions. It did not mention the overdose. He thinks this happens a lot.
"I think this is a similar subject to abortion in the 1960s. Everybody was trying not to see the problem, they were kind of sweeping it under the carpet. They didn't mind it happening so long as it wasn't public and did not rise to the surface," Valentine says.
Another doctor. Another death. A Melbourne GP who does not want to be named says she had known a woman for about a decade when she came to her one day feeling breathless. Scans revealed terminal breast cancer that had spread to her lungs.
After seeing an oncologist, the woman told her GP that she had no interest in letting the tumours slowly claim her life. Instead, she had one request: A syringe pump with enough morphine in it to die gently with her family around her.
"She was a charge sister, a nurse, she was used to controlling other people's lives and she wanted to control her own," the GP says.
Over the following days, the GP spoke with the woman's siblings who understood their sister's view and supported her decision.
By the end of the week, the family was gathered in a small private hospital room. The GP prescribed enough morphine for 24 hours that could be used in one hit. When she left, the woman said goodbye to her loved ones, pushed the pump repeatedly, and slipped away in a deep sleep.
The next day, her siblings visited the GP to thank her.
"They said it was lovely and that they would never make any trouble about it because they understood that that was clearly what she wanted," the doctor says.
"I personally think this is happening all the time, it's just that the media are not hearing about it."
Like Mrs Valentine, there was no mention of suicide or euthanasia on her death certificate.
While all of the doctors who spoke to The Age say it is shameful that seriously ill people do not have equal access to doctors who will help them end their lives peacefully when the time is right, they believe secretive and unregulated assistance has its dangers, too.
For some, this was recently highlighted by the Medical Board of Australia's suspension of Philip Nitschke's registration to practise medicine. Nitschke says the board took the action against him because of discussions he had had with Nigel Brayley, a 45-year-old man who sought his advice while police investigated the suspicious death of his wife. Brayley was not physically ill when he took his own life earlier this year and there are now suggestions he was depressed at the time.
"There needs to be some control over it and at the moment we're getting into a situation where the means are there and uncontrolled," Benson says.
As for the man wanting to mercifully kill his mother, Benson believes it was right for him to offer the advice he gave. He says the woman had clearly stated her wishes to him and that her son was grateful for the conversation, even if it left him in an invidious position.
"I had known both of them. It was not a situation of knocking off mum for her millions. And why knock off mum for her millions? She was going to die within six months anyway. She may have been a burden, but it was obviously a very temporary burden," he says unapologetically.
"I try to do the best for people ... but best to my mind does not necessarily mean living as long as you possibly can. If life is intolerable and you know it's not going to get any better then there's no point in persisting with it."
Benson does not know what happened to the woman and her son in the end, mainly because the pair were living together in another state. He says their situation highlights the unfortunate reality of limited end-of-life choices in Australia.
"This is a big issue and it's about choice," he says. "It's not about forcing anybody to do anything. It's about giving people the option if they need it. Lots of people would like to know it is available."
For help or information visit beyondblue.org.au, call Suicide Helpline Victoria on 1300 651 251, or Lifeline on 131 114
Sunday Age letter:
Yet another account of grudgingly dispensed pain relief (Letters, 31/8). Such behaviour flouts the intent of the Medical Treatment Act – that all patients are entitled to "receive maximum relief from pain and suffering".
Three measures would improve the situation:
1. The state government should clarify the law regarding death resulting from end-of-life pain medication.
2. Care facilities and physicians with a religion-based, pain-relief policy should inform intending patients of their approach.
3. Those of us who would want maximum pain relief throughout should make sure we have advance healthcare directives in place, plus a trusted someone with medical power of attorney to demand it.
But it's a pity the palliative care and dying with dignity movements seem at odds. Basically they are on the same page except for the final paragraph. That's the part that wants to grant the desire of some to leave at sunset, and not go on into the darkness – as Dr Rodney Syme put it so well (Opinion, 17/8).
Anne Riddell, Mt MarthaThanks to the courageous doctors speaking out in support of voluntary assisted dying (''Hiding death from the law'', 7/9). What a contrast to responses I received to a letter I sent in early May to 14 state Coalition and Labor MPs, asking whether they supported voluntary assisted dying in principle. I received six responses. The three from Coalition ranks were brief and cold; ''a proposal for legislation was extensively debated and defeated in the previous Parliament … no plans to legislate on this issue''.
Three responses from Labor members were disappointingly identical in their pro forma wording, emphasising support for expanding palliative care services, and for statutory recognition for advanced directives regarding a future condition, but no support beyond these provisions. One added a brief sentence of in principle support for voluntary euthanasia.
I applaud the doctors for their humanity, but am ashamed of the lack of courage of our parliamentary representatives in spite of the public's high level of support for voluntary euthanasia.
Anne Marsden, Princes HillThe concern is not that doctors, surprise surprise, are driven by compassion to break the law. The concern is the inequality of access to this assistance. It's pot luck as to whether a dying person with untreatable suffering can ask and receive the means to die with dignity, or whether they suffer needlessly through their last days or weeks. If other medical relief from suffering were subject to the same random whimsy there would be outrage. Perhaps parliamentary silence on this matter is because the dead do not vote; but it does remain for those who love family who have died to lobby their MPs to change this law. This is urgent, as the issue is before the Senate.
Janine Truter, The BasinIt is interesting that in all the articles about euthanasia there is always a line at the end giving contact details for Lifeline and the Suicide Helpline. Even if the article seems to favour individuals taking responsibility for their own end-of-life decisions, contact details are never given for Dying with Dignity.
Al Rozefsky, MansfieldLetter in The Age:
Liberal MP Craig Laundy may have given an explanation for why politicians are reluctant to reveal their stance on voluntary assisted dying (Letters, 21/9). Mr Laundy withdrew his public support for a free vote on same-sex marriage because he believes that conscience voting leads to pollies being subjected to vigorous lobbying to make them ''vote against what they believe''. As if we really know what pollies believe!
But this is a democracy. How else are we to know who to vote for unless candidates state their beliefs? And as the dying with dignity movement gathers momentum, many votes will be won or lost on it. Older citizens, in particular, will rate this issue above most others when deciding who should represent them. While a pro-choice belief may be to no avail if a party executive forbids conscience voting, we can still hope enlightened pollies will courageously cross the floor to the side of the angels.
Anne Riddell, Mount MarthaArticle in Sydney Morning Herald:
By Vanessa DesloiresControversial euthanasia campaigner Philip Nitschke has accused the Senate of shutting him out of an inquiry into a proposed Dying With Dignity law.
Dr Nitschke said that neither he nor his recently formed Voluntary Euthanasia Party were asked to speak at a hearing for the inquiry in Melbourne on Wednesday, despite representing the "largest and only national pro-euthanasia organisation in Australia".
The founder of Exit International blamed Greens senator Richard Di Natale, who has proposed the Dying with Dignity Bill, for the exclusion, and was angry that groups who had made "uncharitable and incorrect statements" about him in their submissions were invited to speak.
It comes after the Medical Board of Australia suspended his licence to practice medicine due to concerns he supported the suicide of a man who was not terminally ill.
He was also recently criticised by The Australian Medical Association, Dying with Dignity Victoria and beyondblue.
Article in the Sydney Morning Herald:
By Julie-Anne Davies
Life changer: Peter Nugent will be defending voluntary euthanasia campaigner Philip Nitschke in a hearing before the Medical Board of Australia. Photo: Wayne Taylor
When Melbourne lawyer, Peter Nugent found out a year ago he was dying, his life changed in almost every way, for the better.
The 53-year-old husband and father of two teenagers has colon cancer that has spread to his liver; survival rates say only six per cent of sufferers are alive five years after diagnosis. Nugent hopes to be one of those fortunate few but he isn't wasting time wondering.
On Monday, in a courtroom in Darwin, Nugent will defend the world's most famous and controversial euthanasia campaigner, Philip Nitschke, against serious allegations levelled by the Medical Board of Australia. It suspended Nitschke's medical registration in July in order to "protect public health and safety" after he admitted that he had supported a 45-year-old Perth man's decision to commit suicide, despite knowing the man was not terminally ill. Fairfax understands the board will argue it was forced to use its special emergency powers to protect vulnerable suicidal people from Nitschke and his "dangerous ideas". More seriously, the board will argue, it had to act because Nitschke possesses the means to transform these ideas into action.
These ideas revolve around his view that rational suicide is an acceptable choice for competent adults who may or may not be not suffering from a terminal condition. Nugent, who until now has spent the bulk of his 20 years at the Victorian Bar working almost exclusively in commercial law, had never met Nitschke until three months ago when he contacted him after reading about his suspension.
"It seemed to me Philip Nitschke was a doctor in desperate need of a good lawyer," Nugent says. He says he felt compelled to help Nitschke because to do nothing seemed "gutless".
"It's because of people like Philip that I have options about my end of life. I think it is extraordinary that the board is trying to rub him out because of an idea.
"We are not talking about the state euthanising people. This case is about whether rational adults should be given access to information which could be used to engage in a lawful act – suicide. On one side of the debate is the Medical Board which says doctors know best. On the other side is Philip Nitschke who believes competent adults know best. That is what will be on trial in Darwin next week."
The hearing, before a five-member panel is set down for five days. It is understood the board's lawyers will argue that Nitschke's euthanasia book, The Peaceful Pill Handbook is a practical guide to different methods of suicide and although it is banned in Australia, it is available over the internet without any controls over who accesses it.
Further, it is believed the board will argue that Nitschke informs and updates ebook subscribers of overseas suppliers of the illegal drug Nembutal and through his workshops advises people on end-of-life drugs.
A longtime, fervent supporter of voluntary euthanasia and rational suicide, Nugent isn't looking for end-of-life advice himself because he has already done his own homework. "I will make my own decision when enough is enough, for anyone else to have a say about how my life ends seems ridiculous."
As part of his cancer treatment, he has seen a psychologist who has assured him he is not depressed. His wife Debra and children, 16-year-old Bridgit and 13-year-old Caillin, know his views on end of life but he does not discuss with anyone what he may choose to do himself one day.
"I'm protecting my wife by not talking about my own circumstances," he says. "I don't intend, whatever I do, to involve anyone else, which is sad because I would much prefer to be with my family. If I do make a decision to end my life, I will have to die alone."
He has taken two weeks off chemotherapy treatment to represent Nitschke, although he hasn't told his oncologist his reasons. Some of his colleagues at the Bar are astonished that he has taken on Nitschke, perhaps used to Nugent's dispassionate advocacy in cases that are usually fights over money.
"My daughter said this was the case I was born to run, it's just taken me a very long time to get around to it," he says.
Nugent still feels well enough to work although concedes that 12 months of chemotherapy minus the next fortnight, has robbed him of energy. He doesn't know how many more cases he has left in him but he is prepared to continue to represent Nitschke if he'll have him. "Philip is going to need some legal advice in every state and if he would like me to work with him I'd be delighted."
The Age Editorial:
Today, The Age calls on Federal Parliament to recognise in law the right of terminally ill people to choose, under rigorously regulated circumstances, the timing and manner of their death. In coming hours, the cross-party Senate legal and constitutional affairs committee is expected to report on such a legislative proposal by Greens senator Richard Di Natale. Throughout this week we will be publishing, across our digital platforms and in our newspaper, stories, interviews and arguments to ventilate the case for change, and we invite our readers to participate in the debate in the pages of the paper and online.
The committee may well raise a small number of concerns, but we believe, as other nations have shown, it is eminently possible to produce a law with adequate safeguards. And we believe the moment has arrived for our lawmakers to respect a position surveys have long shown is supported by as many as eight in 10 of our citizens.
We hold that life is inestimably precious and should be protected. But we recognise there are many terminally ill people who suffer dreadfully. In such cases, we share the view of Dr Rodney Syme, one of the leading proponents for physician-assisted death and a man who openly admits to having helped terminally ill people die by giving them the means and knowledge to end their suffering. He is doing so for Peter Short, a Melbourne man close to death who has been campaigning for the right to choose and who is one of the people who inspired Senator Di Natale's bill. A video interview with Mr Short, who testified before the Senate committee, is part of our coverage this week.
Dr Syme's argument, based on decades of experience, is compelling: dying may be associated with excruciating suffering, and there may be a crescendo of suffering as death draws nigh; a doctor's duty is to relieve suffering; some suffering will only be relieved by death; a doctor's duty is to respect a patient's autonomy; some patients rationally and persistently request assistance to die; and, palliative care cannot relieve all the pain and suffering of dying patients. Palliative support is central to our advocacy – most people who have the option of physician-assisted death do not take it, but as Dr Syme, Mr Short and many others attest, those who do have that option immediately benefit because it alleviates fear and anxiety.
Some argue that people might unduly make such a final decision because they are depressed or feel they are a burden to others, and that unscrupulous relatives might seek to manipulate a patient. Overseas experience suggests these concerns are misplaced. Another issue the committee report might raise is definitional boundaries. What should be the definition of terminal, for example? We believe settling this is also readily within the capacity of our lawmakers.
As we have stressed in the past, we do not support voluntary euthanasia advocate Dr Philip Nitschke, because through his organisation, Exit International, he aids people who are not terminally ill to die by suicide, and we are concerned he is fuelling inappropriate demand – and an online black market – for a particular drug being used to induce death. It is in the public interest to pass a law that permits medical practitioners such as Dr Syme to offer peace to terminally ill patients but prevents those like Dr Nitschke from facilitating the death of people who should instead receive treatment.
The time has come for Australia's political leaders to not only grant a conscience vote, but to urge their colleagues to advance our civilisation by passing well-honed legislation. This issue concerns all humanity. It transcends party politics, and it behoves our elected representatives to show courage and decency by delivering an enlightened, compassionate change.
Article in The Age:
By Julia Medew
Liberal Senator Ian Macdonald. Photo: Alex Ellinghausen
By his own admission, veteran politician Ian Macdonald is a "nasty shit" in federal parliament, but he quickly loses his trademark belligerence when discussing his late mother, Gladys.
After chairing a committee examining a new voluntary euthanasia bill, the Liberal Party senator says his mother's prolonged demise has partly shaped his view that terminally ill Australians should have a right to die, provided a law has adequate safeguards in it to protect vulnerable people such as those with mental illnesses.
In a candid interview, Senator Macdonald, an Anglican, said his beloved mother lived for seven years in a Queensland hospital after a severe stroke paralysed her right side in 1983, robbing her of most of her mobility, speech and quality of life.
Despite teaching herself to write with her left hand and to say "yes", "no" and "I love you", six years after her catastrophic stroke she indicated she had had enough.
"There came a stage where she started spitting out pills… but they sort of stood there and watched her take them," he said.
After that tactic failed, she started to refuse food and water. But it took seven months of starvation for her body to finally give in.
"She effectively starved herself to death… That is not a nice way to go," he said.
"At the end, I can remember the doctor saying to Mum 'It's time now Mac, isn't it?' and Mum gave her a sort of weak nod, and then she (the doctor) did something, I'm not sure what."
Senator Macdonald does not want to comment on what that action might have been or whether it hastened his mother's death because he knows there is a grey area for doctors who want to relieve people's suffering at the end of their lives without being seen to euthanase them.
In Australia, it is legal for doctors to use potentially lethal doses of drugs at the end of life, provided their primary intention is to relieve pain. But it is also illegal to assist a suicide, so doctors risk prosecution if they provide fatal doses of drugs to people wanting help to end their lives.
Senator Macdonald does not know if his mother would have qualified for euthanasia under the current "dying with dignity medical services" bill being proposed by Greens Senator Richard Di Natale, but says that if he found himself in her position, he would want a doctor to help him die peacefully when the time was right.
"Putting myself in my mother's position, I would have liked to have been able to accept the inevitable and do something about it," he said.
Under Senator Di Natale's draft bill, adults who are suffering intolerably from a terminal illness and who are mentally competent would be able to request voluntary euthanasia. They would only be given assistance to die if two doctors agree their illness is terminal and a psychiatrist rules they are not suffering from treatable depression. A Senate committee, chaired by Senator Macdonald, has been examining the bill and is expected to table a report about it in parliament today (Monday).
The report comes as prominent euthanasia advocate Philip Nitschke's appeal against a Medical Board of Australia decision to suspend his registration begins in Darwin today. It took the action after Dr Nitschke admitted supporting a 45-year-old Perth man's decision to suicide, despite knowing the man was not terminally ill.
Senator Macdonald, an MP for 24 years, has made headlines in the past for his outspoken and recalcitrant ways.
He became a leading internal critic of John Howard after the former prime minister dropped him from his ministry. When Mr Howard offered him a diplomatic posting, Macdonald reportedly told him to "shove up it his arse".
In December, Senator Macdonald also took a swipe at Tony Abbott's chief of staff, Peta Credlin, by saying the PM's office seemed to "have an almost obsessive centralised control phobia".
Senator Macdonald acknowledged he was best known for his unpleasant personality in parliament, but said this issue appealed to his softer side.
"I'm an aggressive shit when it comes to the parliament… but in these sorts of things, I'm a real softy," he said.
Article in the Sydney Morning Herald:

Though they have different views on the right to die, Labor MP Terri Butler and Nationals Senator John 'Wacka' Williams agree politicians should have a free vote on the issue.
Federal MPs should have a free vote on euthanasia, a Senate committee has recommended.
Tabling its report on proposals to legalise voluntary euthanasia drafted by Greens Senator Richard Di Natale, the Senate Legal and Constitutional Affairs Committee said that if a bill on the issue of euthanasia was introduced in the Senate, party leaders should allow Senators to vote according to their consciences.
A Senate committee has recommended federal MPs be allowed a conscience vote on any voluntary euthanasia put before Parliament.

Senator Di Natale's bill, which he has not formally introduced to the Senate, would make it legal for medical practitioners to help a terminally ill, mentally competent adult end their life.
In what constitutes the first consideration by Federal Parliament of national euthanasia laws, the six-member committee, which includes three Coalition, two Labor and one Greens Senator, recommended Senator Di Natale address several technical concerns, including about the definition of a terminal illness, before taking the bill further.
Senator Di Natale called on Prime Minister Tony Abbott and Opposition Leader Bill Shorten to grant their members a conscience vote.
"The community strongly supports this reform and it's time for politician's to listen," Senator Di Natale said.
"The Committee's report has highlighted some areas that need further discussion, which I intend to do with parliamentary colleagues from all sides before proceeding with the bill."
In 1996, party leaders granted MPs a free vote on a private members bill introduced by Liberal frontbencher Kevin Andrews to override Northern Territory laws which legalised euthanasia. The Andrews bill passed both houses of parliament, overturning the NT laws.
Article in the Sydney Morning Herald:

Appeal: Philip Nitschke's conduct is under scrutiny. Photo: Glenn Campbell
It seemed fitting that euthanasia campaigner Philip Nitschke should be fighting for his medical licence and his professional reputation in the town where he first shot to world attention.
On Monday in Darwin, Mr Nitschke began his appeal in the Northern Territory Civil and Administrative Tribunal against the decision by the Medical Board of Australia to suspend his registration after he admitted supporting a 45-year-old Perth man's decision to commit suicide.
The case was not about voluntary euthanasia nor rational suicide but "a very precisely focused interim hearing into Mr Nitschke's conduct into the death of a man", Ms Lisa Chapman SC for the Medical Board of Australia told the hearing.
In emails between Mr Nitschke and Mr Brayley, Mr Nitschke chose to be registered as a doctor, Ms Chapman said.
"If he hadn't, the board would have no jurisdiction [to suspend his licence]."
Ms Chapman said the emails contained very specific information about various ways to commit suicide.
"The gas flow, where to buy the cylinders from. How to take the peaceful pill.
"He obtained scant information about Mr Brayley before he died."
Before Monday's hearing, Mr Nitschke's barrister Peter Nugent told Fairfax the appeal as "the trial of a dangerous idea".
"It is a controversial subject," he said. "Mr Nitschke is a controversial figure.
"The views which he holds are not abhorrent, they're not out there, they are not even out of step with mainstream Australia's view."
On Monday afternoon the board conceded Mr Nitschke was not in a doctor/patient relationship with Mr Brayley.
Fairfax understands that the board will argue it was forced to use its emergency powers to protect vulnerable suicidal people from Mr Nitschke and his "dangerous ideas". More seriously, the board is expected to tell the five-member panel, it had to act because Mr Nitschke possessed the means to transform these ideas into action.
The hearing is set down for five days. It is understood the board's lawyers will say that Mr Nitschke's euthanasia book, The Peaceful Pill Handbook, is a practical guide to different methods of suicide, and while banned in Australia it is freely available through the internet.
Further, it is believed the board will argue that Mr Nitschke updates e-book subscribers of overseas suppliers of the illegal drug Nembutal, and through his workshops advises people on end-of-life drugs.
Mr Nitschke told Fairfax the opportunity for people to choose to end their life needed to be "enshrined as an option".
"Individuals in a society must have the ability to make decisions over their own lives. Life is a precious gift and so we need to be able to fight for that option."
The hearing continues.
Letters in The Age:
My brother has been bedridden since March dying of brain cancer. My mother has dementia and is fearful every moment as everyone is a stranger. My brother is grateful for any time he has; and my mother had always indicated she did not agree with euthanasia. That is their choice and I respect it. However, watching them both dying has made me determined that if I end up in an agonising, drawn-out death, I want my choice for when and how I die respected, too. It frightens me that I will have no choice and may experience 10 years of dying hell. Everyone tells you how palliative care is so good these days. Nobody mentions the distasteful real difficulties, like bleeding bowels, repeated explosive diarrhoea and having to be dosed up on Valium so you don't scream or abuse people. Opposers of euthanasia make dying sound so fun and cosy. I am discovering just how cosy it really isn't.
Name and address withheldWhat becomes of me when I can no longer feed myself, toilet, clean and dress myself? I may be in my 90s, have lived a long and fulfilling life but can no longer do all of these basic things. I do not want my children to watch me become a shadow of my former self. I want to be able to choose. I want a compassionate GP who, knowing my expressed wishes, is free from litigious risk. My GP can say "she has lived a good life, let's not prolong it any further". What are my chances?
Judy Tolson, KewAs an atheist, I found myself in the interesting position of agreeing with Christian John McClean that "personal autonomy is not enough for a good society" ("The tragedy of physician-assisted suicide", theage.com.au, 10/11). A good society needs a foundation of shared moral values, not just maximal freedom to do whatever an individual chooses. But dying with dignity is not just about individual choice. It's about a society based on compassion and respect. That respect includes not imposing religious views on those who don't believe in God.
Dr Meredith Doig, St Kilda EastThe Age says it's about the right to die. I say that position is based on the assumption that we own our own lives. I don't believe that. After all, I didn't come into this world through my own efforts but as the result of the gift of life given to me. My death is in the hands of a mystery far greater than The Age's understanding of this world and what it means to be human. And what place and meaning suffering has in human life.
Phillip Turnbull, Cornelian Bay, TasmaniaCongratulations on your campaign for federal law reform to support all Australians who want voluntary assisted dying to be available to themselves and loved ones . . . and for emphasising that such a measure will certainly not support Philip Nitschke's "come one, come all" approach to assisting suicides. Many ill and elderly people belong to his Exit International simply because it offers the only prospect of avoiding prolonged pain and indignity before death. If they knew they could rely on being helped to die in certain defined circumstances (which they would have documented ahead of time), then they would not be thinking of a DIY method. If medically assisted dying in tightly controlled circumstances becomes lawful then the demand for personal supplies of Nembutal and other means of suicide advocated by Dr Nitschke is likely to substantially lessen. However, until then, it's understandably a growing market.
Anne Riddell, Mount MarthaArticle in the Sydney Morning Herald:
Parliamentarians from both sides of politics declared their support for voluntary euthanasia on Tuesday, following a Senate report that could pave the way for a free vote on national right-to-die laws.
Labor's deputy leader Tanya Plibersek and former Howard Government Minister Mal Brough were among MPs to add their voices to calls for dying with dignity reform.
Their comments follow the release of a multi-party Senate committee report on Monday that recommended party leaders allow MPs a free vote on euthanasia.
The Senate Legal and Constitutional Affairs Committee, whose six members included three coalition Senators, recommended a conscience vote following an inquiry on the first proposals for national euthanasia laws, put forward by Greens Senator Richard Di Natale.
Senator Di Natale's draft bill would make it legal for medical practitioners to help a terminally ill, mentally competent adult end their life.
Federal Parliament has been asked to consider the issue of euthanasia just once before. In 1996, it voted for a private member's bill introduced by Liberal frontbencher Kevin Andrews to overturn Northern Territory laws that legalised euthanasia. On that occasion, both major parties granted their MPs a free vote.
Whether coalition MPs would be granted a conscience vote on national dying-with-dignity laws remains to be seen.
Prime Minister Tony Abbott, in China attending the APEC summit, was not available to comment on the approach the coalition would take to such a bill.
A spokeswoman for Justice Minister Michael Keenan said:
"There is currently no legislation before the parliament on this matter. Should there be legislation presented in the future, it will be dealt with by the party room in the usual way."
Nationals Senator John Williams said while he opposed euthanasia, he supported a free vote.
"This is a contentious issue, a sensitive issue and a religious issue," he told Fairfax Media. "I personally would not support it, but I have no problem with a conscience vote."
Labor MPs automatically have a conscience vote on euthanasia.
Labor's deputy leader Tanya Plibersek said "I support voluntary euthanasia with appropriate regulation and safeguards," a view reinforced by her experience of watching her father Joseph die slowly and painfully from cancer in 2012.
Liberal MP Mal Brough, who voted against the Andrews bill in 1996, said while he had not seen the Di Natale bill, "I support the notion of dying with dignity."
A spokesman for the Leader of the House, Christopher Pyne, said he did not believe euthanasia should be legal.
Nationals Senator Barry O'Sullivan, a member of the Senate committee that examined the Di Natale bill, said he was "seriously opposed" to euthanasia because he believed the state should not involve itself in matters of life and death.
"Once you legislate for voluntary euthanasia on certain terms, over time it stands to reason that these terms can be expanded or broadened. I think we should stay right out of the space," he said.
Liberal Democratic Party Senator David Leyonhjelm said his party supported euthanasia for people of sound mind as long as their choice was totally voluntary.
"We take the view that if suicide is legal – and it is, and so it should be – it's not moral to deny people assistance to commit suicide just because they're too feeble to do it for themselves," he said.
"We just don't think the government has the right to tell you that you have to stay alive if you are determined not to stay alive. It's not the government's business," Senator Leyonhjelm said.
Senator Di Natale will consider issues raised by the committee with a view to introducing an improved bill, co-sponsored by MPs from other parties, in the first half of 2015.
For help or information call Lifeline on 131 114 or beyondblue on 1300 224 636Article in The Age:
By Julie-Anne Davies
Speaking out: Catherine Ringwood, who is dying of cancer. Photo: Angela Wylie
The desperation of the dying is something Melbourne woman Catherine Ringwood knows intimately. Much of her adult life has been spent in its company, first as a nurse then later as a counsellor for the pro-euthanasia organisation, Exit International.
It became personal 15 years ago when she was diagnosed at just 49 with leukaemia. Since then, Ringwood has fought hard for her life: chemotherapy, radiotherapy, then a mastectomy five years ago after an out of the blue breast cancer diagnosis and finally, gratefully, as a human guinea pig in a cancer drug trial.
A month ago Ringwood, now 64, was told by her doctors at the Peter MacCallum Cancer Centre that the disease was back for good. "The drugs aren't working any more and even though I am a positive person, I know I am pretty much out of medical answers," she says. "I feel some trepidation and obviously a great deal of sadness but I am also so glad I have thought deeply about how I want to die and had the conversation with those I love.

Philip Nitschke with his 94-year-old mother, Gwen, who wants to die.
"If I get to a point where I'm unable to walk, toilet myself, live independently then this would be unacceptable and I would choose to die."
Like many living with a terminal illness or with incurable suffering, maintaining control over their life – and death – is the most important thing.
Her decision to speak publicly about her own end of life plans is crazy-brave in the current climate.
Since April police have raided homes of Exit members in South Australia, Queensland and Western Australia, searching for the banned euthanasia drug, Nembutal. A few weeks ago, a Victorian couple had a surprise visit from two Australian Federal police officers after Customs intercepted a parcel from Thailand containing a banned drug.
"Let them put me in jail, a lot of people in Exit are frightened but not me – can you imagine? Terminally ill woman in jail for victimless crime. Let them try," Ringwood says. Even so, her "action plan" is a secret and she makes it clear, she isn't about to jeopardise that.
"I have the 'information' I need to make my own end of life choice and that's what is keeping me sane right now," Ringwood says. "It would be a major catastrophe if that was taken away.
"Having a plan means that one day, I can give my hematologist a hug and thank him. I've never discussed this with my doctors though, because I am frightened they will say I'm depressed, and feel its one more thing they have to try and fix."
Information, knowledge, action plan, peaceful pill are all euphemisms used by scared, often terminally ill or elderly but sometimes perfectly well people as code for Nembutal. It is the holy grail of the voluntary euthanasia movement used here by vets to put down animals and by legal euthanasia programs in Europe to end the lives of people. It's the drug that turns otherwise law-abiding people into drug smugglers, death tourists, law breakers.
At the beginning of the 21st century, advances in medical technology have made it possible to maintain life where it was previously impossible. But those advances have pushed us into new medical, moral and ethical territory. With the use of sophisticated life support systems, is life being sustained or is death being deferred?
It is an issue many liken to the abortion debate of the 1960s and one which the medical profession, the church, hospitals, nursing homes, and parliaments as well as the broader community, is being forced to confront.
All agree the rights of the dying is the hot ethical debate of the times and will only intensify as the pro-rights baby boomer generation finds itself facing death.
There have been attempts at law reform in every state and territory bar Queensland. In 1996, Australia became, briefly the first jurisdiction in the world to legalise euthanasia for the terminally ill. It was overturned nine months later by the Howard government.
Now, a Greens-sponsored draft dying with dignity bill is winding its way through the committee process of the federal Parliament. It is the first federal attempt at legislation. One of its architects is South Australian GP turned senator Richard Di Natale. He says the time has come for an honest national conversation on end of life choices.
"Look, we know its happening in an unregulated space behind closed doors so there is a strong argument to say lets do it openly and try and break down some of the taboos around death and dying," Di Natale says.
Nearly two decades of reporting from the frontlines of the euthanasia debate has taught me that fear of dying, not fear of death, is the issue that motivates ordinary people to do extraordinary things. Stashed bottles of barbiturates, clandestine trips to dodgy Mexican border towns, failed suicide attempts, money lost in scam internet deals.
Fear of pain, but also the indignity of being trapped in a body which no longer functions but where the brain is as active as ever, can transform the most law abiding and conservative citizens into fugitives.
Not all people interviewed for this story were prepared to be identified. They don't want to risk having their drugs found, scared relatives alerted or their doctors tipped off.
One couple - we'll call them Carol and Bill - are in their 60s and in good health, and say they recently imported cyanide from Thailand after researching the subject carefully.
This is a new and alarming development in the euthanasia drug black market. Testing showed the drug was not pure and so Carol and Bill, like informed consumers, complained to the supplier and another package was sent.
They say they are being responsible by planning for their future and liken it to writing an advance care directive or taking out life insurance.
"We're not alone, many of our friends feel the same way," Carol says. "It's our generation I guess, we're not used to having to put up with pain, we are used to choice. Its interesting how many people have made their plans, equipped themselves and now can get on with their lives."
Her own mother committed suicide by drinking Nembutal just before her 90th birthday. "She was not sick, she was not depressed, she just decided it was time to die. It was not a secret, we all knew her feelings because she valued life, she had meditated on this decision for a very long time. It was a textbook case of rational suicide."
But Carol's mother died alone. She rang her daughter after she had swallowed the medicine but no one was home.
"She left a message on the answering machine saying she was sorry, she was tired and it was time to go. She was protecting us to the end by not involving us. I just wish she hadn't had to go through that last hour alone."
Earlier this year a fascinating correspondence took place between the former chief minister of the Northern Territory and passionate voluntary euthanasia supporter, Marshall Perron, and the South Australian coroner, Mark Johns.
Perron wrote to all Australian coroners seeking their views on what he termed "an unrecognised phenomenon in Australia ... the growing incidence of rational suicide by the elderly and the terminally and hopelessly ill". He was trying to gather some facts to support his contention that too many ill people are choosing to end their life prematurely and alone while they are still physically or mentally able.
"There is anecdotal evidence that such disguised deaths occur regularly..." he wrote.
Only Johns replied. "Much of what you say is quite correct and accords with my own experience," he said. " I agree that these deaths are a sad reflection on our society and the choices that many elderly people face...
"Whilst many coroners might privately agree that voluntary euthanasia ought to be available, coroners, like other members of the judiciary, should not involve themselves in political debates that are as hotly contested as that one. "I do agree that the public is generally unaware. They rely on the people they elect to lead them to inform them of such matters and instigate debate."
Dr Rodney Syme has just come from the bedside of a terminally ill man who took his life the night before. Syme offers few details because he is aware that the police might turn up asking impossible questions of a grieving wife.
"I was there because I'd offered to support this person and to make sure the process went OK. We had a long conversation for an hour and half, going over it all again and then he took the medication and it was all over in about 20 minutes. I spent another three quarters of an hour with the wife talking over what had happened and she offered me a glass of scotch and I had it."
Suicide is not a crime in Australia but assisting someone to die is. Is just being present a felony? "The police have told me its not but aiding and abetting, for example handing someone a drug to take, is illegal," Syme says.
Personally, he has been goading police to arrest him for years. He admitted giving Nembutal to former Victorian journalist Steve Guest in 2005 while he was dying of esophageal cancer but the police have said there is not enough evidence to press charges.
Dying with Dignity Victoria – Syme is vice president – represents the mainstream "physician assisted dying" side of the debate which is the position the Greens draft bill espouses. They want law reform so that doctors who currently work in the murky grey zone of "terminal sedation" can practice without fear of prosecution. And the terminally ill and chronically suffering can have a peaceful, painless death at a time of their choosing.
"Medical assistance at the end of a person's life is just good palliative care," Syme says. "It's not illegal to commit suicide, to refuse medical treatment including refusing artificial food and fluids, to ask for medical treatment to be withdrawn – there is only this missing bit at the end – to allow people a dignified death with assistance by a doctor."
Gwen Nitschke wants to die but the very last person who can help her is her son, Philip Nitschke, the world's most controversial voluntary euthanasia advocate and, currently, a suspended doctor fighting for his medical registration and reputation.
It's deeply ironic that the 94-year-old, who has lived in a nursing home in Adelaide for the past six years and is still sharp as a tack, wakes up every morning and announces to the world that she wishes she was dead. Her son, who has written the book on ways to die as well as being the first doctor in the world to practice legal physician-assisted dying, cannot help her.
Gwen is not terminally ill, she is like so many elderly Australians, slowly dying. She can't move about without using a walking frame or wheelchair and she is lonely; living to nearly 100 means she has watched most of her friends go first.
"I am tired and I just want this to end," she says in a phone interview the week before her son's appeal against his suspension.
"I wish I'd done something earlier to help send me on my way but I left my run too late."
Nitschke says his mother feels stranded. "The weekly visits out to the nursing home are invariably difficult, stressful and hard going for her and us. Waiting is a form of suffering and that's what she is doing. I feel quite sad that I can't give her the drugs, I feel upset by her situation. She looks at me each time and says the same thing. 'It's just my luck to have you as a son'."
theage.com.au/comment/righttodieThe Age letters:
My great-grandfather Alexander Syme and his brothers Ebenezer and David, who established The Age in the 1850s and 1860s, would be proud of the modern Age in carrying on their tradition of challenging parliament to represent the wishes of the majority of citizens. The right of citizens to have a choice as to how, when and where they die has long been a wish of the vast majority of citizens. The law affecting how doctors engage with their patients at the end of life is vague. Doctors do help their patients to die in arbitrary and clandestine circumstances – the authorities know this, but do nothing about it, unless someone complains. "The rule of law" is lauded as a jewel of our culture, yet it means that some suffer grievously while others escape, based on whom they know, their disease, their social circumstances and their knowledge, courage and energy. Change this law, for all our sakes.
Dr Rodney Syme, ToorakThree years ago my 76-year-old father died of cancer. He spent his last six weeks unable to move from the waist down but able to experience pain throughout his body. He screamed with pain; begged to die. Once, after awaking from a morphine-induced sleep he thought his granddaughter was an angel and asked her to swing his legs to the ground so he could walk away from his life and his pain. When he realised he wasn't dead his anguish was heart-breaking. He shouldn't have had to endure such agony.
Jennie Hartwell, BeaumarisThe term "conscience vote" suggests that members of parliament should only consider their own beliefs when deciding how to vote on an issue ("Call for MPs' euthanasia conscience vote", 11/11). But as the representative of an electorate they should also consider the views of the voters in their electorate. With about 80 per cent of voters in favour of euthanasia in certain circumstances how can a MP justify ignoring their constituents? Party leaders can tell their MPs they may vote as they wish but they can not tell them to just ignore their electorate. We should just call it a free vote.
Peter Hogan, Clifton HillTaking one's life or being assisted to do so is not an act of courage, but one of denying the very autonomy and dignity that is being claimed as justification for being able to choose, since it denies the absolute worth of a being capable of such powerful decision-making. In destroying ourselves, we seriously weaken the justification for regarding ourselves and others with respect, because we have placed limits on our self-worth, and by implication that of others, by regarding some kinds of life as not worth living. We come into the world dependent on others and leave it dependent on others. Our infirmity, no matter how severe, does not diminish our worth; our last obligation is to affirm this, not only for ourselves but also for others.
Professor Janis Ozolins, Australian Catholic UniversityPhillip Turnbull (Letters, 11/11) intimates that life, death and dying (often with pain, indignity and suffering) are simply part of a bigger (presumably "God's") plan. What a cop-out. We may well be born "without any efforts of [our] own" but part of the gift we are given is a trait called personal responsibility; it is that part of us that allows us to "own our own lives". People who are suffering must not be arbitrarily inhibited from exercising their ultimate personal responsibility. Let's leave religion, spirituality or any quaint notions of wondrous mystery out of what is an essentially biological, physical and emotional problem.
George Petrides, BelgraveArticle in The Age:
Illustration: John Spooner
In May this year, in these pages, Peter Short wrote a forthright opinion piece declaring he was dying of oesophageal cancer, had a supply of Nembutal and would end his own life at a time of his choosing. In January this year, his doctors gave him six months to live. He is still very much alive and is campaigning vigorously for the passage of legislation that would make it easier for people to do what he declares he will do: choose the manner and timing of their own deaths over medically protracted indignity and suffering.
I am writing to add my voice to the chorus calling for this serious matter to be addressed in such a way that we can create a new and better code of civilised norms around suffering, medicine and death. I am not terminally ill and I do not have a supply of Nembutal. I do, on the other hand, have metastatic melanoma. That means that my health and general viability are an ongoing experiment, at the cutting edge of current medical science. The debate about euthanasia hovers – and must be conducted – at the cutting edge of moral philosophy.
We dwell, I think, more in stories than in systematic arguments when it comes to death and dying. When I contemplate the possibility of freely embracing and actively triggering my own demise, three stories are foremost in my mind. Two of them are historical and of those, one far better known than the other. The third is from a highly popular work of fiction by a devout Catholic writer and all the more remarkable for that reason.

Remarkable storyteller: Author J. R. R. Tolkien was a deeply moral Catholic, but he had one of his most exalted characters choose to lay down the gift of life in order to avoid the infirmities of old age.
The first story is that of the death of Socrates, in 399BCE. (I write BCE, Before the Common Era, not BC, before Christ, since this is a moral dialogue in which only some of us are Christians). He was condemned to death by the state for corrupting the youth and encouraging atheism. His friends urged him to escape and flee Athens. He chose instead to take his hemlock and pass away. Was he wrong to do so? He famously remarked, as his vitality ebbed away, that he owed a cock to Asclepius – as if his death had cured him of an illness. Certainly, he died with lucid dignity. Bettany Hughes provides a fine account of both his life and death in her 2010 book The Hemlock Cup: Socrates, Athens and the Search for the Good Life.
The second story is one related by the Roman historian Tacitus in Book XI of his Annals of Imperial Rome. It concerns the death of a wealthy Gallo-Roman aristocrat, Valerius Asiaticus, whose opulent villa and gardens were coveted by the dissolute Messalina, mistress of the Emperor Claudius. She had false charges of treason brought against him and he was condemned to death, but was permitted to choose the means of his own demise. The historian recounts "he took his usual exercise, then bathed and dined cheerfully and ... opened his veins, but not until he had inspected his funeral pyre and directed its removal to another spot, lest the smoke should hurt the thick foliage of the trees. So complete was his calmness even to the last."
The third story is buried in Appendix A to J. R. R. Tolkien's The Lord of the Rings. It concerns the voluntary suicide of Aragorn, 120 years after the fable ends. Having lived a long life, he announces to his beloved Arwen that the time has come to lay down the gift of life and leave the throne to their son. She begs him to linger with her and not go before his time. His response is remarkable: "Not before my time," he answered. "For if I will not go now then I must soon go perforce ... Take counsel with yourself, beloved, and ask whether you would indeed have me wait until I wither and fall from my high seat, unmanned and witless. Nay, lady, I am the last of the Numenoreans and the latest King of the Elder Days; and to me has been given not only a span thrice that of Men of Middle-earth, but also the grace to go at my will and give back the gift. Now, therefore, I will sleep."
That phrasing is worth dwelling upon: "the grace to go at my will and give back the gift". That, I suggest, is the tone in which to think about our ends – not a tone or language of fear, anxiety and a ban on choice. But all three stories inform my sense of what it could mean to voluntarily bring an end to one's own life and to do so in a dignified manner. Should I reach the point where an ending seemed more dignified than enduring, it is stories such as these that I would bear in mind.
The chief source of our ban on voluntary euthanasia is in the Catholic tradition, dating back not to scripture, but to St Augustine. He rejected the Stoic and the Epicurean approach to free death. Yet Tolkien, a deeply moral Catholic, had one of his most exalted figures choose to lay down the gift of life simply in order to avoid the infirmities of old age. He was being neither frivolous nor sinister. He plainly conveys, in his telling of the story, the sense that this was a lofty freedom available to the "latest King of the Elder Days" and that it made good sense. The need, in whatever set of laws we frame around medicine and mortality, is for civilised norms. All three of these stories, I believe, show that voluntary death can be experienced and conducted according to civilised norms. At the very least, they exhibit norms in which the emphasis is on choice and dignity, not a fearful ban on freedom of action. That is the spirit in which we need to frame our laws. That is the calmness and dignity we need.
Paul Monk is an author, former senior intelligence analyst and commentator on public and international affairs.


"I'm not switching off": Exit International's Philip Nitschke. Photo: Getty Images
Euthanasia campaigner Philip Nitschke will consider abandoning his right to practice medicine, he has told a Darwin tribunal.
Dr Nitschke said he was fighting a decision by the South Australian medical board to suspend him primarily to defend his reputation and right to fair process.
The Board used emergency powers to suspend Dr Nitschke after media reports he supported a Western Australian man, Nigel Brayley, who was not terminally ill but had decided to take his own life.
Police were investigating the murder of Mr Brayley's wife when he died. He had also been involved with another woman who disappeared.
Dr Nitschke earlier told the hearing he had no obligation to encourage people who want to end their lives to seek help, even if they do not have a terminal illness.
Barrister Lisa Chapman, acting for the Medical Board of Australia, asked Dr Nitschke whether or not he believed if a person who wanted to commit suicide due to financial difficulties or being tired of life should be directed towards a doctor and be examined for depression.
He said if someone approached him at a meeting of his euthanasia group Exit International and said they did not have terminal illness but wanted to end their life, he would ask them why.
"It's not for me to come along and second judge and, if you like, frustrate or thwart that person's plan for their future," he said. "[But] the reason is relevant - if they said they were going to suicide because it's the end of the world tomorrow, I would of course engage further.
"To try to draw this connection, this one-on-one connection, that every person who suicides is somehow the victim of a mental illness, is simply incorrect."
Dr Nitschke told the tribunal he spends most of his time now doing advocacy work, and has only treated about six patients in the past two years, of whom two were new patients.
He said if a patient said they wanted to end their life, he would assess them for depression and refer them on for further help - because they had come to him as a patient seeking treatment from a doctor.
But he believed people with a depressed mood or elements of depression, as long as they were not psychotic or severely mentally impaired, could make an "informed decision" about ending their lives.
Ms Chapman asked him how he could just "switch off" his role as a doctor when acting as a political advocate. "I'm not switching off ... you are effectively saying, because I'm a doctor it must be a medical assessment [when I meet people at Exit International meetings]," he said, adding that such meetings usually involved about 300 people and only cursory meetings.
The president of the tribunal, Kelvin Currie, asked Dr Nitschke if he had become desensitised to the experience of being told by someone that they were considering suicide.
"It's obviously not a normal experience. I recognise the emails I get every day are not normal emails," Dr Nitschke said. "It takes away the alarm reaction that people who don't see these emails often get ... and I behave in such a way that some would see as insensitive."
The tribunal heard that when Dr Nitschke heard Mr Brayley's life was not "going well" he initially asked him if he wanted to talk about it, or wanted to talk to a medical professional.
But later, during an email exchange, when Mr Brayley indicated he was planning to kill himself soon, Dr Nitschke did not repeat the suggestion he get help. Mr Brayley asked if Dr Nitschke would like to receive a copy of his suicide note, and he said yes.
The medical board maintains that the code of conduct for doctors means they have an obligation to the health of individuals and society at all times.
"You would expect a doctor to conduct his or herself according to that particularly high standard in their general lives," Ms Chapman told the tribunal.
The hearing continues.
Lifeline 13 11 14Letters in The Age:
My husband, Robert, advocated physician-assisted dying. He suffered bulbar-onset motor neuron disease and likened its symptoms to the tortures experienced at Guantanamo Bay: stress positions, sleep deprivation, waterboarding (choking), personal humiliations and, worst of all, the existential suffering of an indeterminate sentence. He faced a death of asphyxiation through choking or lung paralysis. Palliative care is excellent but cannot relieve all suffering of the terminally ill. The choice of the time to die belongs to the sufferer alone. Feeling a burden to others is often just an additional torment for someone already suffering multiple afflictions. Robert had professional support, loving family and palliative aids. He also had the respect of those who accepted his need for dignity in dying.
Robert took his own life in 2009. Countless others have since experienced a horrific dying process or taken their lives through violent means, their only solution. Meanwhile, our politicians prevaricate, refusing to recognise that legislation with rigorous safeguards can be enacted. Legislation offers release from suffering, not continuation of torture; it offers not only dignity but compassion.
Nica Cordover, Allens Rivulet, TasJanis Ozolins argues that if we choose to end our life we deny our intrinsic worth (Letters, 12/11). He even implies that choosing to die is cowardly – an insult to the many worthy people who have ended or wish to end their life in the face of intolerable suffering. By "life" Ozolins, like so many opposed to voluntary euthanasia, has in mind some abstract concept, not the lived embodied life of real people in extremis.
To have become sentient in an otherwise possibly blank universe is a miracle. But it does not follow that our life is not our own; what would be the point otherwise? While infirmity does not diminish our intrinsic worth, nor does the wish to end our life in certain situations. There is a curious taint of moral blackmail about this argument and an accompanying want of empathy for others.
Michael Read, AshburtonI respect people's right to believe in any religion they choose. In return I expect the religious to refrain from foisting their beliefs on me; but this is repeatedly shown to be a forlorn hope. Few, if any, arguments against end-of-life decisions are not primarily based upon religious beliefs. If the religious want to prove their worth by suffering unspeakable pain and indignity at the end of their lives, go ahead; but please do not demand that I suffer to make you feel better.
Ian Smith, WhittleseaThe issue of physician-assisted suicide is often conceptualised as an argument between religious and non-religious views, and considered on an individualised, personal basis. However the consequences of such legislation on the common good must also be considered. Your editorial (10/11) advocated legislation allowing physician-assisted suicide with adequate safeguards: the difficulty is there are no such safeguards. There is no way of protecting vulnerable people from zealots who have an obsession with facilitating death, or doctors who cannot properly assess ill patients. Elder abuse is increasingly recognised and older people are vulnerable to gaining the impression from others that they are a nuisance. Indeed, indications for euthanasia in the Netherlands and Belgium have widened to include non-terminal patients and depressive illness. Palliative care may not be perfect but it is better than the alternative.
Dr John Buchanan, Surrey HillsArticle in the Sydney Morning Herald:


Medical dilemma: Dr Janey Sklovsky believes the law prevented her from carrying out her mother's wish to die with dignity. Photo: Chris Hopkins
Shortly after Janey Sklovsky's mother took her last breath, Janey picked up a camera and started photographing Celia's emaciated body.
Like a forensic expert at a crime scene, Janey walked around her precious mum, taking close-ups from various angles to document exactly how she looked when she died.
Having slowly starved and dehydrated to death with Alzheimer's Disease, Celia was curled up in the foetal position on her left side. Her pale cheeks were hollow, her mouth open; her eyes strained and bloodshot.

Suffering: Celia Sklovsky in her final days.
After months of lying mostly still in bed, her muscles were stiff and her skin paper-thin. Despite the best of care, pressure sores around her bottom were starting to crack open.
"I photographed her because I thought this should not happen to anybody - it was horrible," Janey says, holding the pictures that are now etched in her mind.
In some ways, Sklovsky, a GP, felt like a crime had been committed against her mother and, as a doctor and holder of her mother's medical power of attorney, she felt implicated.
After Sklovsky gained her medical degree in 1975, she says her mother repeatedly told her she did not want to be kept alive if she ended up in a situation where she had gone "gaa gaa", felt useless and had no quality of life.
"I'd rather be driven off the Great Ocean Road," the paid-up member of the voluntary euthanasia society kept saying before she got sick.
At first, dementia seemed to be kind to her in some ways. It made Celia forget the sadness of losing her beloved husband Gresche who died suddenly from heart failure aged 79.
But, over time, the disease started to make the usually calm artist angry, aggressive and paranoid. At times, she thought Janey was a thief who had broken into her home.
It also robbed her of her independence. She forgot how to look after herself, requiring a nurse to live with her at her Camberwell home, and arthritis and osteoporosis stopped her from walking and tending to her beloved garden. Janey remembers the pain of watching her try to paint in the studio behind her grand old Victorian-era home.
"It was tragic, she would just stare vacantly because she had forgotten how to mix paints," Janey says. "On days when she had insight, that was incredibly distressing for her."
By the time Celia was 86, Janey says she appeared to have lost most of her enjoyment in life. Despite having a loving nurse who fed her mostly oysters and eskimo pie ice-creams (the only things she would eat for the last year or so), Janey says all she could do was lie in bed and stroke her nurse's two dogs.
By this time, Janey says she had decided not to do anything to prolong her life. She stopped getting her mum flu injections and did not treat infections in the hope they might gently take her life.
But Celia's body persisted against the odds until she was 89. One day in the winter of 2014, she stopped eating and drinking - a change that coincided with her organs shutting down.
For four days, she took no nourishment. Janey ensured she was kept comfortable with strong painkillers until she died. She could have given her mother a lethal dose of the morphine she had on hand to keep her comfortable, but felt restricted by the law banning euthanasia.
"What could I do? I had a family to support and a professional life. I did not need to be dragged through the courts," Janey says.
Sklovsky is one of a growing number of doctors who say they are frustrated by the current laws governing end-of-life care in Australia. There is, they say, a significant grey area between what is considered good, legal medical care, and what is regarded as unethically helping a person to die in a way that could be considered murder.
At the moment, doctors can legally do a range of things that may hasten someone's death. They can stop life-prolonging interventions such as pacemakers, they can decide not to initiate life-prolonging measures such as antibiotics to treat an infection, and they can administer potentially lethal doses of drugs like morphine to relieve severe pain at the end of life. All of these things are permissible if the primary intention is to help the patient, even if the "secondary consequence" might be death.
This means that every year, many people who are dying in hospitals or palliative care units are given "terminal sedation" or large doses of painkillers to relieve their suffering while dying, even though they might speed up death.
But for some doctors, this is not enough to relieve the psychological and existential pain some people may feel when dying. If those people want to control their end by staying at home, for example, and don't want to suffer catastrophic pain that might warrant a lethal drug in a hospital at the very end, there are no legal medical options for them to end their own life.
For more than a decade, Melbourne urologist Rodney Syme has been privately helping people overcome this. Syme, the vice-president of Dying with Dignity, says he provided many terminally ill people with advice on what they can do to end their own lives at the time of their choosing. In April, Dr Syme toldThe Age that he had provided Victorian Steve Guest with a lethal drug that he used to kill himself. Guest had been dying of oesophageal cancer and did not want to be hospitalised when he took his own life at home in 2005.
The admission was risky. Syme was trying to goad police into charging him with an offence in the hope it would lead to a test case that will be judged in his favour. If he was charged with assisting a suicide and found guilty, he could be incarcerated for up to five years.
While the police have interviewed Syme over his public confession, no charges have been laid so far. Syme believes this is because of a "benign conspiracy" among law enforcement authorities who do not want to prosecute such cases because they can see the mercy involved.
But organisations that regulate doctors and hear complaints against them are taking notice of doctors who sail too close to the law.
Earlier this year, a GP who "over-prescribed" morphine for two palliative care patients at a Sydney nursing home was suspended for six months and banned from working in nursing homes and palliative care units thereafter.
The Medical Observer reported that in the final days of two patients' lives, the GP prescribed intravenous doses of morphine that exceeded accepted therapeutic amounts. One of the patients was in a permanent vegetative state after a stroke and was in severe pain from a gangrenous toe. The other had peripheral vascular disease, renal failure and Alzheimer's disease.
The doctor told the NSW Health Care Complaints Commission that she had made a mistake and was impaired by undiagnosed depression at the time. But in its judgment, the commission said the GP had appeared confident when a nurse questioned her prescription for one of the patients and it was therefore not convinced her actions were the result of mental ill-health. It is not clear if the morphine hastened the patients' deaths or not.
The Medical Board of Australia also recently used its emergency powers to suspend the medical registration of euthanasia campaigner Philip Nitschke this year after he admitted advising a Perth man on suicide, even though that man was not terminally ill and possibly depressed.
While many doctors say they are already helping terminally ill patients die - a 2007 survey of 854 Victorian doctors found that about 100 had agreed to a request to hasten someone's death by giving them drugs - many powerful organisations representing doctors, such as the Royal Australian and New Zealand College of GPs, do not support the legalisation of voluntary euthanasia.
The recent federal government inquiry into a draft "dying with dignity" bill proposed by Greens Senator Richard Di Natale flushed out the views of more than a dozen doctors and groups representing the medical profession. Under the bill, which Senator Di Natale says he will refine for a conscience vote, someone with a terminal illness who is suffering intolerably would be able to ask for help to die.
To qualify for a prescription of a lethal drug, two doctors would have to agree the person was suffering a terminal illness and a psychiatrist would have to rule that they did not have treatable depression.
But the most influential doctors' union, the Australian Medical Association, does not support it. In a submission to the inquiry, the AMA said doctors should not be involved in interventions that have as their primary intention the ending of a person's life. It said this conflicted with the basic ethical principles of medical practice.
Other individual doctors echoed this point in submissions, saying such a law would undermine the healing reputation of the medical profession and trust in them not to hurt or damage their patients, as espoused by the ancient Hippocratic Oath.
Some feared such a law would bring out the worst in people. One Sydney surgeon Robert Claxton said he was concerned that medically assisted suicide would be a "great temptation to a cash strapped health department" and an "irresistible temptation" to those seeking to inherit money from relatives.
Palliative care physicians protested against it, too, saying it could undermine the provision of their services which can relieve physical pain for up to 90 per cent of people at the end of their lives.
One pair of palliative care specialists said legalising voluntary euthanasia could make their services become a "hurdle" that needs to be crossed to get an assisted death when more funding for palliative care would actually reduce the perceived demand for assisted suicide and euthanasia.
Another doctor who works in the Northern Territory, Teem-Wing Yip, said she was concerned about how such a law would affect Aboriginal Australians who suffer from high rates of incurable diseases and are often encouraged to receive treatment from doctors they do not trust.
Dr Yip said her patients often hated the interventions used to keep them alive, such as kidney dialysis, and occasionally said they did not want to live. Some were grateful, though, for the extraordinary measures used to prolong their lives.
She feared the legalisation of euthanasia would require a large amount of resources to educate Aboriginal people about the laws to alleviate mistrust in doctors and said this money would be better spent on preventing diseases in the marginalised population.
But Dr Christopher Ryan, a psychiatrist at the University of Sydney's Centre for Values, Ethics and the Law in Medicine supported legalising euthanasia because, at the moment, there was a contradiction in the way end-of-life care was carried out.
"It seems to me that when things get really desperate we're happy enough to kill people but we have to wait until things are desperate, and then we're not necessarily asking the person, we're sort of deciding for them which seems not quite right to me," he says.
While others say such a law would undermine trust in doctors, Dr Ryan said the status quo arguably discouraged honest conversation with patients who don't think they can ask for help to die because euthanasia is illegal.
There is also a fundamental inequity, he says, because well connected people such as doctors and their families can find assistance to take their own lives gently in the face of imminent death, while others go on without a choice.
Sklovsky says it has taken her about a decade to start remembering her mother as the loving, fit, independent woman she was before her illness. In many ways, she thinks her mum lived for three years longer than she would have wanted.
Sklovksy says drafting laws will inevitably be difficult, but it is wrong that doctors abiding by the law at the moment are often causing more suffering.
"If you can be charged with cruelty to an animal, I think I could have been charged with cruelty to my mum," she says.
"If I had kept my dog in the condition, I think it would have considered unacceptable. But this is what happens in civilised Australia. This is what happens because I didn't want to risk my career."
LINKS
Red Jos: HUMAN RIGHTS ACTIVISM
Mannie and Kendall Present: LESBIAN AND GAY SOLIDARITY ACTIVISMS
Mannie's weblogs may be accessed directly by clicking on to the following links
Activist Kicks Backs - Blognow archive re-housed - 2005-2009
RED JOS BLOGSPOT (From January 2009 onwards)
This page created on 15 NOVEMBER 2014 and updated 7 JULY 2021
PAGE 85