

Article from the Sunday Age:
It is because people do not let go easily that we need more control of how we die. IT WASN'T the other ''bread and butter'' issues that animated the eight women I overheard last week in a cafe in rural Queensland. In their late 50s and 60s, the women were talking about euthanasia.
They avoided the ugly word that conjures images of Nazis. But how to die with dignity was on their mind. ''I wish the politicians would get on with it,'' one said. Another replied, ''Don't wait for them; when the time comes, just do it.''
Some of the women had mothers, aunts or relatives in their 90s, it transpired, and some had friends or relatives dying of cancer. Tony Abbott claims the euthanasia debate is low priority.
But he is wrong. How to die with dignity is a subject of keen interest to an ageing population that has witnessed extraordinary gains in longevity often accompanied by great suffering. If these women are any guide, the subject of a good death is a concern felt well beyond caffe latte suburbs.
Death once came quickly to most people. Previous generations were taken out by infections, childbirth, pneumonia, heart attacks. How to die was never a problem when the period between diagnosis and death was short, leaving just enough time for goodbyes and last rites. People still die suddenly in their sleep, in the shower, at their desk or on the road. But they are more likely to die slowly - from cancers, organ failure or the multiple infirmities of old age. The wonder is that those in the firing line, with terminal illnesses or in extreme old age, more often than not rage against the dying of the light. In coffee shop chat, when one's own death seems remote, it is easy to say, ''When the time comes, just do it''.
But for many with incurable diseases or extreme age, the impulse is to fight. It is not a death pill they clamour for but life. They never give up hope. They try experimental drugs and complementary medicines. Having so far survived breast cancer, I can testify how a glance with death keenly sharpens one's appetite for life.
The old and the terminally ill will put up with a lot to hold on. They treat death as the enemy. This leads some to overestimate the time they have left and put off hard conversations. But the indomitable will to live is the best safeguard against misuse of euthanasia laws. It is precisely because people don't let go easily that state and federal governments should introduce laws that give people greater control over how they die.
Some people finally reach a point where the suffering becomes intolerable; they fight for every breath, their physical pain cannot be relieved; their anguish cannot be dispelled with drugs. They fear an undignified, lingering end. Palliative care, as wonderful as it can be, is not enough for 5 to 10 per cent of dying people, and morphine, even at very high doses, does not always conquer pain.
When incurably ill people of rational mind decide that life has become too gruelling, no one should tell them they are wrong, least of all outsiders who seek to impose their religious views on others. Knowing how furiously people cling to life, a request for a peaceful, dignified and easy death should be respected.
It is not beyond governments to frame safe laws. Oregon's Death with Dignity Act is 13 years old. Hedged with many safeguards, it could act as a starting point. Doctors prescribe medication on request to qualifying people judged to have six months to live. But control over if and when to ingest the medication is left with the individual. In about a third of cases, people never take the prescribed medication.
The Oregon law has not led to a ''slippery slope'', nor put vulnerable groups, including the poor, at heightened risk. It has been used by a tiny minority, accounting for 460 deaths over 12 years out of 360,000. Palliative care has not been undermined.
As more baby boomers, like the Queensland women, witness the long and lingering deaths of elderly parents and not-so-elderly friends, the clamour for some form of physician-assisted death will grow.
Most people will never need to take the prescribed medicine that would take them from consciousness to death in five minutes or so. But knowing such an end was within their control would ease for many dying Australians the terror of letting go.
Adele Horin is a Fairfax staff journalist.This letter in The Age 290910 is problematic for a number of reasons, the main one being that the letter-writer states that she has changed her mind since originally supporting the Northern Territory's legislation to bring the Bill into being, but not giving reasoned explanations as to what her objections to euthanasia legislation would be if introduced by the federal parliament in 2010 or 2011. More rational discussion is required before her simplistic explanation has any credence.
IN THE 1990s I worked as a doctor in Alice Springs in the Northern Territory and contributed to bringing the bill supporting euthanasia into legislation.
Philosophically, there seemed to me to be no reason why people who have a terminal illness needed to suffer longer than they wanted. However, I have changed my view.
Since 2001 I have worked at The Gawler Foundation with thousands of people affected by cancer and multiple sclerosis. As a consequence, I caution anyone who thinks that euthanasia is a simple matter of human rights.
Many of the patients I have known are in shock or depressed, and are particularly worried about the burden that they are to their families, emotionally and financially. Initially, these people are often confused in their thinking.
At a time where we are all concerned about the burgeoning aged population, as well as overpopulation, the clarity about who actually wants to die and what reason is a good reason, becomes fraught.
With my experience, I have changed my view completely, and no longer believe that it would be safe to legalise euthanasia.
Dr Ruth Gawler, The Gawler Foundation, Yarra JunctionLetter in The Age newspaper:
RUTH Gawler has used her famous name to deal readers a specious argument (Letters, 29/9); her failure to grasp the essential part of euthanasia puzzles me. Medicine has enabled the old to live way past the time when people used to die.
Many doctors have mistakenly used this as an excuse to mend the broken bodies of the dying; to prolong, with no cessation of pain, life without any chance the patient will regain a decent existence. Operations are carried out that do nothing to enhance a patient's life, but make a nice living for the doctor.
To suggest the dying are using euthanasia as a form of civil rights may suit Dr Gawler. It does nothing to enhance the lives of the dying.
Venise Alstergren, ToorakLetters in The Age newspaper:
IF WE are going to discuss euthanasia, it is not enough to simply tell moving stories where a loved elder in terminal discomfort is kindly granted release by a caring doctor (''Our fierce will to live holds key to debate on euthanasia laws'', 26/9). We have to talk about what would happen if we changed the law.
Human beings sometimes act out of love, but sometimes out of greed, revenge, laziness, self-pity or self-interest. The law has to deal with human nature as it is. Every effort should be made to avoid creating a bureaucratic procedure that authorises doctors to end life.
Our first priority should be to remove the pressure for euthanasia. This means good-quality palliative care, an acceptance that humane pain relief may collaterally shorten life, and sensible hospital policies that spare the dying from the use of extraordinary technology to uselessly extend a terminal stupor.
PHILIP O'CARROLL, North FitzroyEUTHANASIA must be an individual decision and not only for the terminally ill; quality of life is another aspect that must also be considered. While life may be sacred for some people, it may no longer be sacred for others, and just because some people want to live forever does not give them the right to determine that everybody else has to feel the same way.
''Freedom of choice'' means nothing if everyone insists on making the choices for you. Every person must be given the right to live, or to die, with dignity.
The time has come to introduce an independent board of doctors who will assess all applications to ''die with dignity'' and who must first take into account all past, present and future aspects of the life of the applicant. For the terminally ill, decisions should be made swiftly but for those who no longer believe they have ''quality of life'', a further similar application to the board six months later would confirm their application and should appease those who have objections to euthanasia.
Everyone has to die and nobody likes grieving, but death, with its associated grief, is inevitable. Why should people who are living only to get out of bed in the morning in order to return to it at night be forced to live, just to keep other people happy?
NOLA MARTIN, PrestonLIKE many who support euthanasia, Adele Horin claims those with ''religious views'' are imposing themselves on the dying. While many hospitals and palliative care facilities are run by those of religious views to help the sick and dying, Horin does not recognise that she is equally ''imposing'' her view. She is seeking a shift in the paradigm in dealing with death.
One would be naive to think that euthanasia is just about giving ''free choice''; our decisions are made in a social context that gives and privileges some options over others. Allowing euthanasia privileges a certain option and creates social pressure through a certain message: a ''good death'' is not about facing everything life gives you (with and for others), but about ''choosing'' when I want to die.
Of course, we all fear pain and sympathise with those who undergo it, yet asking society to participate in killing does not respect life or relationships. Our will to live is not just natural, but also socially formed. Respecting and enabling the will to live (among the young and old) involves seeing life through, not cutting it off.
DR JOEL HODGE, systematic theology lecturer, Australian Catholic UniversityArticle in The Age newspaper:
A PIONEER of Belgium's voluntary euthanasia law has rebuffed Prime Minister Julia Gillard's statement that it could be ''almost impossible'' to find appropriate safeguards for such a law in Australia.
Professor Jan Bernheim, a cancer specialist who was instrumental in creating Belgium's voluntary euthanasia law in 2002, said Australia could learn a lot from his country about how to create a safe system.
Last week, Ms Gillard said she found it difficult to conceive how there could be appropriate safeguards for such a law, but Professor Bernheim said Belgium's safeguards had worked very well for the past eight years.
''Ms Gillard obviously hasn't looked at the data,'' Professor Bernheim said. ''I think Belgium has a system that is well worth considering.''
He said research showed that before Belgium's law came into effect, about 4 per cent of all deaths involved mercy killing by doctors and nurses - three-quarters of which occurred without any request from the patients.
''If you were in a bad shape and terminally ill, you were more likely to get physician-assisted death if you did not ask for it than if you did,'' Professor Bernheim said.
''If you did ask, the family and nurses would know about it and then there would be a risk of somebody suing the doctor. If you did not ask for it, it was mercy killing by the doctor, so this was an intellectually and ethically distasteful situation … There were no safeguards at all.'' He said a survey of doctors done in Australia in the late 1990s showed a similar level of clandestine mercy killings.
Under Belgium's law, about 2000 people have volunteered to be euthanased each year. All of these terminally ill patients met strict criteria, including tests to ensure they were cognitively competent and that their disease and suffering was irreversible. Suffering is defined as both physical or psychosocial pain.
According to the law, the patient's request has to be constant and repeated with no evidence of coercion. The request must be reviewed by the patient's doctor, as well as an independent doctor who has not been caring for them.
If it is granted, the doctor who administers the lethal injections must stay with the patient until they die.
Professor Bernheim said Belgium's euthanasia law was introduced alongside another law that doubled funding for palliative care services - a move he views as crucial to its success.
He said although most palliative care physicians initially opposed euthanasia because they feared it might be viewed as a substitute for palliative care, this had not eventuated, and the majority of these doctors now supported the law.
Professor Bernheim, who is also a researcher with the End-of-Life Care Research Group in Brussels, will address the biennial conference of the World Federation of Right To Die Societies in Melbourne this week.
Meanwhile, lobby group Exit International has been given the go-ahead to erect Australia's first pro-euthanasia billboard, on the Hume Highway in outer Sydney.
Lawyers from Billboards Australia, owner of the proposed site, had feared it could be illegal. It is an offence under New South Wales law to incite or counsel a person to commit suicide. However, Exit argued successfully that the ad contained no incitement to suicide and was simply an expression of the public support for voluntary euthanasia.
The ad will be on the billboard from October 11.
Article in The Age newspaper:
Opinions are divided on whether euthanasia can be a rational choice.
Bob Brown's post-election call for a conscience vote on the territories' right to pass euthanasia laws has been criticised for being a distraction from issues that really matter to the average Australian.
But such criticism misses the likelihood that the 21st century may well be the one where ''how to die'' becomes as important a question as ''how to live''.
Advances in medical care have transformed our relationship to dying. Medical technology will continue to blur what we mean by death and its relation to our lives, foreshadowed by extraordinary cases such as 41-year-old American Terri Schiavo, who was in a vegetative state for more than 15 years. A prolonged legal and political battle eventually led to the stopping of tube feeding in 2005, and her death.
A much less publicised case was played out in Australia in 2003. The New South Wales Supreme Court ruled that treatment could be withdrawn from Isaac Messiha, a 75-year-old man whose life was supported by ventilation and tube feeding after he suffered severe brain damage from a stroke.
It is a difficult discussion to have in a society that has so little exposure to death and dying in comparison with previous generations. The average young Australian may face death only through their pets or when they travel to other parts of the world, especially countries with Hindu traditions where bodies are sometimes cremated on the street.
Half of all deaths now occur in hospitals, three times the rate of 20 years ago. Several colleagues of mine working in intensive care complain that their job is increasingly about prolonging vegetative states and delaying inevitable death.
The greatest proportion of health costs is in the period surrounding death. Much of it is consumed by machines plugged into electrical outlets - respirators, feeding tubes and defibrillators. The longer we live, the longer we take to die.
While euthanasia is the most discussed, there is a spectrum of actions that hasten death, from withholding treatment to physician-assisted suicide. One that happens every day in hospitals, hospices and nursing homes is when medications such as morphine are increased to alleviate debilitating pain, causing the patient to stop breathing and die. It is something I have undertaken myself.
With the growing pressure on Western health budgets, there is a greater urgency to debate issues such as rational suicide, a controversial topic within psychiatry, a field in which all suicide is generally seen as a disturbance of the mind.
Rational suicide has also been called balance-sheet suicide, suggesting that sane individuals can objectively weigh the pros and cons of continued life, and then decide in favour of death. Views vary from the act being the ultimate expression of one's autonomy to it being morally reprehensible.
Christopher Ryan, a psychiatrist at Sydney's Westmead Hospital who specialises in mental disorders among the medically ill, ensured that the original Northern Territory legislation stipulated a psychiatric review before euthanasia. He believes in the concept of rational suicide but considers it extremely rare. He thinks depression or demoralisation usually overlies the decision.
Physicians, by contrast, appear to believe ill patients often choose to hasten death for rational reasons. Studies in 2008 in Oregon and the Netherlands, regions where euthanasia is legal, show that in the Netherlands only 4 per cent of patients were referred for psychiatric evaluation. The rates were similar in Oregon.
The studies found that physicians placed a greater weight on the importance of existential issues such as loss of dignity and feelings of being a burden. Such feelings have been shown to be particularly relevant to dying patients' will to live.
Studies of dialysis patients show that the incidence of depression was not greater in patients who withdrew from the treatment. A key factor for them was the importance of maintaining control, a finding consistent with many patients in Oregon who chose euthanasia. Doctors working with cancer patients have emphasised similar personality characteristics in patients seeking to accelerate their deaths.
Suicide rates among the elderly in Australia, especially the group over 75 years old, have steadily grown in the past two decades. They are now considered one of the highest risk groups. It is difficult to know what proportion could have been saved with appropriate treatment, as many do not seek medical help.
But while suicides among young people are always considered tragedies, attitudes are more ambivalent about the elderly, suggesting the lay public may have a stronger belief in rational suicide than many mental health professionals.
Western attitudes to death have progressed from it being a public and familiar event, to it being the moment when our souls are up for judgment, to present attitudes of material finality. We need a greater understanding of how and why people make certain decisions surrounding their deaths, not to mention greater reflection on the process itself.
Tanveer Ahmed is a psychiatry registrar and writer.Article in The Age newspaper:
Dr Roger Hunt, director of the Western Palliative Care service in Adelaide, said the threat of a murder charge meant doctors were not talking openly with patients and their families about terminal sedation - the use of drugs, such as benzodiazepines, to induce a coma that eventually leads to death.
He said the laws governing its use meant physicians could only provide terminal sedation to a patient if their primary intention was to relieve suffering, even though it also sped up the dying process. If doctors' primary intention was to hasten death and they told a patient or their family this, Dr Hunt said, they could face a murder charge.
''The current law and the way it's set up around the clinician's intention only encourages less-than-honest expression of what is really happening,'' he said.
''The outcome of hastening death with this treatment is downplayed and often not discussed when it should be. It's sort of wiped away as a secondary, unintended or an untoward consequence that is accepted because the primary intention is said to be the relief of suffering.''
Dr Hunt said that given a 1999 survey of 683 Australian surgeons showed about third of them had given drugs to suffering patients to speed up their deaths, the current laws needed to be reformed. ''If it came to the law's attention, all of those doctors could be charged with murder. That would be a lot of surgeons in jail,'' he said.
Dr Hunt said the threat of prosecution meant some doctors were potentially putting off terminal sedation and not offering it as quickly as they could. Where possible, he said, new laws should take into account the patient's wishes so terminal sedation could be openly discussed and agreed to when the patient felt it was the right time.
''The law needs to set up a framework for ethical clinical decision-making because at the moment it's too narrowly focused on the clinician's intention,'' he said.
''I think a better framework would show that the patient and family's wishes are taken into account and that there is a considered clinical discussion about the best way to proceed.
Those things can be documented and objectively looked at, whereas the intention of the clinician is difficult to prise out of somebody, especially if it's a situation where you say the wrong thing and could be prosecuted for murder.''
In an interview before his speech at the World Federation of the Right to Die Societies in Melbourne today, Dr Hunt said he also hoped to see more choices made available to Australian patients because palliative care had some limitations.
For example, although terminal sedation offered many patients a peaceful end, they could still live for weeks without nutrition or hydration after being sedated. ''It can be a difficult period and some patients would prefer to have a quicker death. It can also be a harrowing time for families as well,'' he said.
Article in The Age newspaper:

FOR the past 13 years, Barbara Glidewell has spoken to hundreds of people who have resolved to die. She describes such people as being ''in the zone … detached, very matter-of-fact''.
''They're looking at you from a whole different perspective; one that isn't ours. I've had the most profound conversations of my life with some of these people. It is a very sacred time for them, a sweet time,'' Associate Professor Glidewell says.
Professor Glidewell, in Melbourne for a conference of the World Federation of Right to Die Societies, is an ethics adviser and retired hospital ombudsman from Oregon in the US, where physician-assisted deaths have been legal since 1997.
She has played a critical oversight role in the process that gives people permission to end their lives. Unsurprisingly, she disagrees with Prime Minister Julia Gillard's concern that a system of proper safeguards to enable euthanasia might be an impossible ask.
To be a candidate for assisted death in Oregon, an individual must be terminally ill, with a life expectancy of less than six months. The patients take part in two interviews, 15 days apart. In the first, the patient meets with a ''willing'' physician to determine whether ''the patient believes the suffering could be so intense that they may wish to hasten their death''.
''The physician will be looking for signs of depression or persuasion so that you are sure that the individual is not under any duress or acting out of compassion for their loved ones.'' Professor Glidewell and the medical staff also look for some evidence that the quest for a dignified death has been an ''enduring value'' for a patient.
The second interview is held to determine whether the patients still feel the same. In the interim, they would have signed the required legal documents in the presence of two witnesses - at least one of whom doesn't stand to gain financially from the death. A second consulting physician would also have filed a report on the patient by this stage. If patients get through the second interview, they're given a script for a lethal drug.
Professor Glidewell says she sees about 25 people a year, although about one-third of patients don't end up using the drug.
She understands the procedure can be confronting to people weighing up the merits of euthanasia laws: ''Look, this [assisted death] is a treatment option - that's how we should look at it. It's just one option for end of life, and we'll never bring it up for them as an option.''
Article in the Sunday Age:
BRITISH actor Michael Caine has said he persuaded a doctor to give his terminally ill father a fatal overdose, adding his voice to the country’s long-running debate about assisted suicide.
The Oscar-winning star of The Italian Job and The Dark Knight said in a radio interview he had kept the secret for more than 50 years and now advocated voluntary euthanasia "where life is no longer bearable".
"My father had cancer of the liver and I was in such anguish over the pain he was in, that I said to this doctor, I said 'Isn't there anything else you could, just give him an overdose and end this', because I wanted him to go and he said 'Oh no, no, no, we couldn't do that,'" he told Classic FM.
"Then, as I was leaving, he said 'Come back at midnight.' I came back at midnight and my father died at five past 12. So he'd done it," he said in the interview.
Caine's father Maurice Micklewhite, a porter at a London fish market, died in hospital at the age of 56 in 1955.
The actor said his father had been given just three or four days to live when he asked the doctor to help.
He said he kept the request secret from his mother, who died in 1989.
Asked if he agreed with voluntary euthanasia, Caine, 77, said: "Oh I think so, yeah. "‘I think if you're in a state to where life is no longer bearable, if you want to go. I'm not saying that anyone else should make the decision, but I made the request, but my father was semi-conscious."
Helping people with terminal illnesses to commit suicide is a hotly disputed topic in Britain, where it remains illegal but is rarely prosecuted.
The issue has been brought into sharp focus by a string of high-profile cases.These included two cases of mothers who killed their seriously ill children, one of whom was jailed and another who was not.
AFPLetter in the Sunday Age:
DR JOEL Hodge (Letters, 3/10) writes in the lofty tones particular to those so comfortably ensconced in the religious paradigm of dealing with death. He simply makes no concession to those many people who do not fundamentally subscribe to the redemptive heroics of Christ-like, cross-bearing suffering. This is precisely why many people seek ''a shift within the paradigm of dealing with death''.
As Dr Hodge points out, our decisions are made within a social context which privileges a certain option. For too long the traditional uniformity of the religious paradigm has been privileged to the express exclusion of anything else, despite the complexities of individual human experience.
Surely as a society of the 21st century we are capable of crafting balanced, compassionate and ethically legitimate end-of-life guidelines, which may or may not include euthanasia, depending on the needs of the individual. No one could argue that this is a simplistic exercise, but insisting on keeping the fact of euthanasia a societal taboo will not make it go away. A ''good death'' is not an unreasonable thing to wish for, and must be defined by the individual facing that death.
MICHELLE GOLDSMITH, EaglehawkAustralian Dying with Dignity groups have joined together in a new national body: YourLastRight.com
Alliance chairman Neil Francis, who launched the group during the World Federation of Right to Die Societies global conference in Melbourne in October (2010), said the group would help deliver aid-in-dying reform to all Australians.
He said parliaments around the country had voted down reforms which were supported by a majority of people.
“Assisted dying law in our land lags monumentally behind the will of its people”, Mr Francis said.
“We pledge to strive in unison and harmony to help achieve what our nation’s citizens want: choice and dignity at end of life for all, not just for some.”
In Western Australia, the Voluntary Euthanasia Bill 2010 was defeated in parliament.
An aid-in-dying bill is currently before the South Australian parliament, while Tasmanian deputy Premier Lara Giddings has said she will introduce a bill in that state and Cate Faehrmann has announced one in NSW.
YourLastRight.com member groups are Dying with Dignity Victoria, NSW, Queensland and Tasmania, and the South Australian and Western Australian and Northern Territory Voluntary Euthanasia Societies.
*Phone (03) 9877 7677Article by Adele Horin in The Age newspaper:
THREE out of four Australians believe voluntary euthanasia should be legal, according to a poll.
But despite levels of endorsement that have hovered between 75 and 85 per cent for many years, pro-euthanasia reformers admit to having been consistently outgunned by their opponents, resulting in five failed attempts to have legislation passed in two years.
The latest poll by the Australia Institute found 75 per cent of people agreed that, if someone with a terminal illness who is experiencing unrelievable suffering asks to die, a doctor should be allowed to assist them to die. Thirteen per cent did not agree and 12 per cent were not sure.
As well, the poll revealed 65 per cent of people who identified as Christians were in agreement, as were 71 per cent of Coalition voters, 79 per cent of Labor voters, and 90 per cent of Green voters.
The deputy director of the Australia Institute, Josh Fear, said the high support among Christians was striking, as was the 73 per cent support from people aged 65 and over.
''If anyone in the community would have thought about it and had strong views, it would be people feeling their mortality,'' Mr Fear said. ''Support in the oldest age group was slightly less than average but still very much a majority.''
The poll of 1294 people was conducted online but drawn from a nationally representative sample. It found 18 to 24-year-olds, with 70 per cent support, had the highest level of ''not sure'' at 16 per cent while the 65-plus group had the lowest proportion of ''not sure'' at 7 per cent.
Euthanasia bills have been voted down in Victoria, Tasmania, Western Australia and twice in South Australia since 2008. Federal Greens leader Bob Brown will introduce a bill to seek to overturn legislation that prevents the ACT and Northern Territory from legalising euthanasia. NSW Greens MP Cate Faehrmann plans to introduce a private members bill in her state parliament this year.
Ms Faehrmann said that despite wide public support she expected a repeat of the forceful campaigning by the Catholic Labor Right and the Catholic Church seen in other states.
''The proposed bill has so many safeguards that only a very small number of patients would be able to access it,'' she said.
''We know from Oregon's experience [that] the vast majority who access the law have no religion. People with strong religious views don't access it and shouldn't stop others from doing so.''
SA Greens MP Tammy Franks said the defeat of a bill last November followed a highly organised and well-resourced campaign by conservatives working together across party, religious, and even state lines.
''Until the voluntary euthanasia side is able to compete with such a highly organised campaign machine we are going to struggle to have the majority voice heard,'' she said.
WA Greens MP Robin Chapple, whose bill was defeated in September, said a well-orchestrated campaign that included a personal letter from the Catholic Archbishop to MPs had been influential.
------- and a letter in response in The Age, 7 January 2011:
AS WELL as showing once again that three-quarters of respondents favour voluntary euthanasia (''Euthanasia wins 75% support'', The Age, 6/1), this survey showed that the over 65s had the lowest proportion who were ''not sure''.
One of the repeated weapons the anti-euthanasia lobby use is the suggested threat to the frail elderly - and yet in reality it is those approaching old age who are the least likely to have any doubts. They face the reality of their own end of life and want choice in the manner and time of it.
As ever, with the safeguards in place, no one would be at risk, but at the moment we are all at risk of having this final decision taken on our behalf by someone else.
Ruth Boschen, BalwynLetter in The Age newspaper:
HOW CAN Paul Johnson (Letters, 8/1) know that the article on support for voluntary euthanasia (The Age, 6/1) presents ''a flawed survey result'' based on ''framing bias'' when its structure and questions are not detailed?
The overwhelming support corresponds with national surveys conducted by organisations including Newspoll, Morgan and Ozpoll. If families who have experienced the unrelievable and protracted death of a loved one could raise their voices (usually they are too distressed to speak publicly), the detractors of choice in dying would hear that ''unrelievable suffering'' is not emotive and dishonest, much less rare.
Judith Hoy, RichmondThe following article is from The Age newspaper:
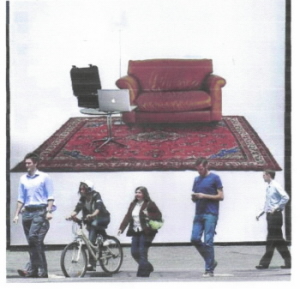
A photograph of My Beautiful Chair hangs from The Republic Tower in Melbourne. Photo: Craig Abraham
IF YOU were faced with the prospect of enduring a painful and protracted death in the grip of a terminal disease, would you want the legally sanctioned option of taking your own life? It is a vexed question that has polarised Australian society. But for artist Greg Taylor the answer is clear.
''Whether I would do it, I don't know, but I would at least want to have the choice. We don't tell people what God they have to worship, that's a choice that they have, so why should they be foisting their choice of death onto us?'' he said.
''Why should we have to suffer as a sacrifice to their God? That's bizarre, especially if you are an atheist. Hey, people, live and let live.''
As you may have guessed, Taylor is an atheist and euthanasia is the focus of his latest artwork, My Beautiful Chair. Some people might not consider it art - but what the work will do, literally, is put people in the hot seat, allowing them to experience what it might be like to choose to die.
Essentially, the work is a cosy domestic setting, the kind that Taylor would want to die in, surrounded by loved ones. There's a plush leather armchair, an elegant floor lamp and an antique Persian rug. On the top of a sleek glass coffee table is a seemingly innocuous laptop and a briefcase.
In fact, the laptop and briefcase are fully functioning replicas of the machine created by Australian doctor and ardent pro-euthanasia campaigner Philip Nitschke to help people end their life.
Euphemistically called the ''Deliverance Machine'', it has also been dubbed ''the laptop of death'' by opponents. When euthanasia was legal for a short time in the Northern Territory in the 1990s, four terminally ill people used the ''Deliverance Machine'' to end their lives.
On Saturday, the public will be able to passively experience what those four people went through, when Taylor's work goes on show in Hobart.
My Beautiful Chair is part of the opening exhibition of what promises to be one of Australia's most controversial private galleries, the Museum of Old and New Art, owned by art collector and professional gambler David Walsh, who knows about the suffering endured by the terminally ill.
Mr Walsh's brother, Tim, died of cancer 19 years ago, aged 33. As his disease progressed, ''he became more humiliated, less my brother'', Mr Walsh says.
Yesterday, a poster of My Beautiful Chair was erected on the Republic Tower billboard, on the corner of La Trobe and Queen streets, which has been the site of some traffic-stopping art, although the significance of Taylor's work may have been lost on passers-by. Its meaning is not immediately apparent.
When Taylor contacted Dr Nitschke to enlist his technical help in the creation of My Beautiful Chair, the doctor was intrigued. Taylor's unusual request came at an opportune time. Dr Nitschke and his organisation, Exit International, had been looking for ways to broaden the debate.
Article in the Sydney Morning Herald newspaper:
EUTHANASIA was contrary to the ideals of justice and charity and would corrupt society, a Catholic bishop has warned the legal fraternity.
The Bishop of Parramatta, Anthony Fisher, used a service at St Mary's Cathedral yesterday attended by the NSW Attorney-General, John Hatzistergos, the shadow attorney-general, Greg Smith, and leading judges and barristers, to warn that ''state-sanctioned killing'' undermined the legitimacy of the state and its criminal law.
''Even were such a proposal to gain a parliamentary majority this would not make it right,'' he said.
Illustration: Cathy Wilcox''Bad laws are mostly made by bad people and in turn make people bad.''
Bishop Fisher called on those gathered for the 81st annual Red Mass, which marks the start of the legal year, to resist efforts to legalise voluntary euthanasia.
The Greens leader, Bob Brown, has vowed to reintroduce a bill to overturn federal legislation that prevents its legalisation in the ACT and Northern Territory.
In NSW the Greens intend to introduce a private member's bill in support of legalising euthanasia after the election in March.
A NSW Greens MP, Cate Faehrmann, said the bishop's comments were an example of an ''out-of-touch commentator driven by out-of-touch ideology''. ''The vast majority of people support voluntary euthanasia as long as it's with appropriate safeguards, which is what the legislation I am proposing is about.''
Bishop Fisher, a former lawyer, said the proposed legislation was ''the killing of those who suffer by those who are comfortable, of the vulnerable by the powerful, of the sick by those professed to heal them''.
''Pope John Paul II went so far as to deem such laws 'lacking authentic juridical validity' and requiring lawyers and health professionals to refuse conscientiously to follow them,'' he said.
That remark echoed comments of Cardinal George Pell in a newspaper interview last month, where he denounced Catholic politicians who defied the church's teachings when considering controversial issues such as euthanasia or same-sex adoption.
The Premier, Kristina Keneally, a devout Catholic, told News Ltd at the time that the cardinal's comments risked being ''interpreted as condemnatory and threatening''.
But she said yesterday she did not personally support the legalisation of voluntary euthanasia.
''As I have said previously, a politician's faith and how they reconcile their beliefs in their public decision-making is a matter for each individual MP.
"The NSW government is yet to see the Greens' proposed legislation and will give it due consideration when it is forthcoming."
When asked if the bishop's comments on euthanasia were appropriate, Richard Perrignon, president of the St Thomas More Society (which sponsors the Red Mass), said the bishop was well-known for his views on euthanasia.
''It's a democracy we live in and people are entitled to their views - even prelates,'' he said.
A spokesman for Mr Hatzistergos, who is Greek Orthodox, referred to comments made in 2002 when he spoke against the Rights of the Terminally Ill Bill. The bill introduced by a Greens MP, Ian Cohen, was defeated.
Letters in response to above article in SMH:
I take great exception to Bishop Anthony Fisher's comments on euthanasia and his pejorative remarks towards those who are in favour of it (''Euthanasia a bad law by bad people, says bishop'', February 1). Legally and medically supervised euthanasia is not ''killing of those who suffer by those who are comfortable''. Any doctor, lawyer and especially family member of a patient undergoing euthanasia will feel the opposite of comfortable and will be acutely aware that a person's death is being caused. But they will be satisfied they are doing something that allows the patient to die without pain and in dignity.
It is not the ''killing of those vulnerable by the powerful''. In fact the process will empower a person dying from an illness over which they no longer have any control, and allow them to have control over the manner in which they die. The ultimate decision will be theirs alone.
It is not the ''killing of the sick by those who profess to heal them''. As doctors we should be there for a patient as much to help them die in peace and comfort when we can no longer do anything for them, as to help them with sickness.
Dr John Frith PaddingtonThe NSW Greens MP Cate Faehrmann suggests Bishop Fisher's comments rejecting euthanasia legislation represent ''out-of-touch ideology''. Yet her own stance, that such legislation is proper because ''the vast majority of people support voluntary euthanasia as long as it's with appropriate safeguards'', seems to suggest that moral issues be decided by popular opinion. So if the vast majority of people think it is OK to diddle their taxes, it is OK to do so. Try that on the Tax Office.
Perhaps Ms Faehrmann could undertake some of the ethics classes being promoted by the Greens. There she might learn that morality is not a matter of majority opinion.
She also might learn to share Bishop Fisher's concerns that euthanasia involves ''the killing of those who suffer by those who are comfortable, of the vulnerable by the powerful, of the sick by those professed to heal them''' and that a society is judged by how it treats its most vulnerable.
Neil Ormerod Professor of Theology, Australian Catholic University, StrathfieldHow on earth can the Bishop of Parramatta argue that even a parliamentary majority ''would not make [euthanasia] right''? Clearly, such a majority would indicate that the moral convictions of Australian society have changed and that morality and law are in opposition to each other.
In Dishonest to God, Mary Warnock says ''a democratically elected parliament is the best interpreter of where the consensus lies''. If not here, where else could it possibly be found?
In the 21st century, the quiet majority of Australians neither expect nor approve of the church leading moral opinion.
Matthew Endacott Brandy HillPurple prose such as ''state-sanctioned killing''' does not embellish Bishop Anthony Fisher's argument against the right of suffering individuals to have their wishes respected. The bishop's lack of reflection on his pronouncement that ''bad laws are mostly made by bad people and in turn make people bad'' is striking, especially given his audience, and the worldwide challenge to the church to properly address the deficiencies of canon law in light of its treatment of young people.
It is here, not in acceding to requests by competent adults, that the suffering of the vulnerable at the hands of the powerful is perpetuated.
Julia Anaf Norwood (SA)Bishop Anthony Fisher is quite right: ''Bad laws are mostly made by bad people and in turn make people bad.'' For example, the Catholic Church's canon law provisions on birth control, women priests, clerical celibacy and homosexuality.
Michael Frawley Downer (ACT)Article in The Age:

MICHAEL SHORT: Rodney Syme, welcome to The Zone. Thank you very much for your time. Spurred by your medical and your human experience, you’ve long held that people must be allowed to die with greater dignity; that under certain circumstances they ought to have the choice to have a medically assisted death. The law leaves doctors therefore in a very difficult position. Can you please talk about what you think ought to be the case, and what is the case at the moment?
RODNEY SYME: What ought to be the case is that if a person has suffering – and that term in the broadest sense to include not just physical suffering, but psychological and existential suffering – that is they’ve got that suffering and it can’t be relived and it’s intolerable, that they should be able to ask a doctor for assistance to end their life. If that’s what’s they want; so this is an entirely voluntary concept.
There should be certain safeguards in law regarding that. People should be carefully assessed. My view is that in that circumstance that I’ve raised there should be a dialogue between the doctor and the person, and as a result of that dialogue it becomes clear, crystal clear, what the circumstances are, what the person wants, whether there is any alternative treatment that could be used to try to alter that person’s situation, to be sure that there are not medical treatments that would have a really good possibility of altering their state of mind, and to make sure that their state of mind is rational. So those safeguards need to be in place.
I think it’s appropriate that a second doctor should verify that that is the case. There needs to be some documentation to see that the person is clearly acknowledging that that’s what they want. That’s basically what the law should allow.
At the present time, the law in my opinion is extremely faulty. What the law says is that it’s a serious crime to intend to end someone’s life or to assist them in ending their life. And it makes no exceptions. We’re all the same. So doctors are treated in the eyes of the law exactly like an ordinary person - other than a doctor.
I don’t mean that other people are not ordinary! It doesn’t recognise that doctors are in an exceptionally difficult position. People expect that doctors will relieve their suffering. Nowhere is that more important than at the end of life. But the law doesn’t protect doctors. It’s what I call one of the medical givens that sometimes suffering will only be relieved by dying. And if that’s the only way it can be relieved then there are arguments that dying should be assisted and brought forward.
But the law makes no exception, and so doctors are in this very, very exposed position. The law somehow subtly acknowledges this and so there are precedents in place that say that if a doctor is intending only to relieve suffering, (and) not to hasten death, then that’s OK. But there’s no clarity in that, there’s no transparency.
And because the law is about a very serious crime it means that many doctors, probably most doctors, have a fear of falling foul of it and having their whole career, their freedom and integrity at risk, their ability to practise their medicine.
And so what it means is that for a doctor to actually help a person, he has to take risks. Now, I think the risks are overblown, because it’s my view that the authorities are not particularly interested in perusing doctors. Nevertheless, that’s what the law says and the way that law in interpreted inhibits doctors from helping people.
So, whether you get help or not depends on a number of arbitrary factors, and it shouldn’t be arbitrary.
MS: I want to come back to some of the things that you talked about in terms of suffering – existential suffering etcetera – and I want to explore a little bit with you the idea of death and how we treat that in life individually and collectively – but while we’re on the law, let’s have a look at some of those things that you’re talking about. You speak of a benign conspiracy. Can you talk a little bit more about that and then we have a look perhaps at the Steve Guest case as a case in point?
RS: Well, I’ve actually been helping people to a dignified death for 34, 35 years. It’s a long time. In that time I’ve probably provided assistance to some hundreds of people.
I sometimes think that maybe people might regard me at Australia’s Harold Shipman, except that Harold Shipman was delivering lethal injections to people he’d see didn’t want them and he had a financial interest in the outcome of the death.
When I first was helping people to die, I was terrified of the authorities. I took enormous lengths to try to keep a space between me and what was happening. But as things evolved, I found that the authorities really weren’t particularly interested in pursuing me.
In 1995, I think it was, I was one of the Melbourne Seven, who revealed that we’d been helping people to die, and the prosecutorial interest in that was like a slap on the wrist with a wet fish. And I thought, `hmmm, that’s interesting’. And I subsequently embarked on a campaign with the coroner to try to establish the reality of terminal sedation, a process where doctors deliberately put people to sleep and keep them asleep and don’t feed them and hydrate them until they die. You can’t tell me that’s not hastening death.
But the coroner really went for cover – wasn’t interested in answering my queries about that. And then finally in 2005, I confronted the authorities over the death of Steve Guest, and again I was interviewed twice by Victoria Police and despite the fact that there’d been significant circumstantial evidence and despite the fact that I think anybody looking at what I’ve said rationally would not think for one moment that I hadn’t provided lethal medication to Steve Guest, the authorities do nothing.
As a consequence, I fell that the authorities do not want to address this issue, and it therefore empowers me to further provoke the matter in the future in all probability.
MS: Now, we distinguish here between the authorities, the people who enforce law, and our lawmakers, the politicians who make law. How far are you prepared go to push this?
RS:With Steve Guest, I’ve indicated that I gave him advice. My original statement that I thought would be appropriate said that I gave him advice that gave him control over the end of his life. Now, you could say that’s a euphemism for assisting him.
Actually, whilst that was true my reason for providing him with medication was to give him control. Giving him control was the best palliation he could possibly have. So whilst on one side you could possibly argue that I was assisting in his suicide, on the other hand I would argue that I’m giving him the best possible palliation – relieving the psychological and existential suffering which was paramount with him.
I subsequently went on to indicate that I talked to him about barbiturates and to state that I’d given him medication. I deliberately have not stated what that medication was. But I have the opportunity to do so and if I do so I think there will be no argument that the authorities have all the information they need to prosecute me.
They haven’t done so, I think because they realise they would lose the prosecution. I don’t think there’s a jury in this country that would convict me of a crime in doing what I did with Steve Guest. I don’t regard myself as a criminal and I don’t think most people would.
And so if parliaments continue to refuse to recognise what the vast majority of people want, then I think the only way to resolve this issue would be through the courts.
MS: And you’re prepared to take that next step and describe the medication?
RS: I am.
MS: To specify the medication to allow a prosecutor to join the dots should one wish?
RS: Yes.
MS: Why do you think that our law makers are so apparently far behind the community and those who are called upon to work within the law and apply these laws? Why are our politicians so far off the pace on this issue?
RS: A very, very important issue is the impact of the Catholic Church, which has a significant power through its organisation, its hold over those people who still devoutly believe what the church says. They have a power to influence people in the ballot box, and if you’re a politician on a one or two per cent margin you might be very fearful of putting your hand up in support.
Secondly, I do think that a number of our politicians are concerned that although the population would want change, they are concerned about whether it can be done responsibly and safely. I think the evidence - the empirical evidence from those countries where this has been done, The Netherlands, Belgium, Oregon, Washington - is that it can be done. But I don’t think they are sufficiently well-informed about this despite everything that proponents of law change would argue.
And of course there’s history, there’s history. There’s a history of the law in this respect: the law is terribly conservative, the medical profession is very conservative. Something that irritates me intensely is the fact that whilst I know that a lot of my colleagues in medicine agree with me, it upsets me greatly that very few of them will put their hand up and say `this is right, something ought to be done’.
There’s a lot of people in the law who believe the law ought to be changed but we don’t hear from them. Politicians ultimately respond to the public and they also respond to critical, intelligent argument, and I’d really like to see more people of integrity stand up and say what they think.
MS: The logical conclusion of what you’re saying, Rodney, is that a change in the law to allow medically assisted death is inevitable.
RS: I think it is, but when I don’t know. One of the reasons why I’ve come to the conclusion that it may need a challenge in the courts to alter this matter is a reflection on what happened with abortion. You reflect on the fact in 1968, Mr Justice Menhennitt effectively changed the practise of the law in relation to abortion and it took the Parliament another 40 years to pass legislation. I think if a judicial precedent were established, it would allow more doctors to practise appropriately and possibly the law wouldn’t take 40 years to change.
MS: Just before we move on from law and politics and how that relates to this issue, are you optimistic about some of the attempts at the state and territory level at the moment in Australia to bring about some change? Western Australia just had a crack – it didn’t go very well. Tasmania looks like it might be lining up to go in that direction…
RS: Yes. I think there have been a number of attempts to change the law through private members’ bills. I’ve looked at them all very closely and some of them are not constructed in the best possible way, and that therefore gives politicians the opportunity to say `well, I don’t think that’s a very good bill; it’s not responsible enough’. And therefore they vote it down.
In Tasmania, Lara Giddings, who has just become the Premier, has together with Greens’ Nick McKim, who may be deputy premier, together have stated that they will introduce legislation in the Tasmanian Parliament. It’s a powerful combination and this is the one thing that’s been lacking in previous attempts at legislation – support from within the parliament; senior people in the parliament taking the initiative to introduce legislation. And that legislation will have all the advantages of parliamentary counsel, serious lawmakers, drawing up legislation. So, I think Tasmania will have a very good possibility of passing legislation.
MS: When they’re drawing up the legislation, where would you urge people doing this drafting to look? You’ve mentioned The Netherlands, Belgium, Oregon and Washington. Where is the best of the statues that you’re aware of? What would be a good model?
RS: I don’t think any of them are particularly good models. One thing both Belgium and The Netherlands have is very simple legislation. It simply creates a circumstance which allows doctors to assist, provided they practise according to the guidelines, and the guidelines are laid down by the medical associations to a large extent.
The thing that’s been lacking in Australia is any support for this from the Australian Medical Association; despite the fact that a lot of polls show that the majority of doctors support it.
MS: They say they’re open to change and open to argument, but it’s clear that the AMA is following, at best, and certainly not leading on this issue.
RS: It is not. The AMA is a somewhat endangered organisation. Its membership has been falling. And it’s very sensitive to doing anything which would threaten a core part of its membership – those members who would be opposed to it – so it sits on its hands. It refuses to have a plebiscite of its members to see what they think.
It relies on the view of a select number of people in the assemblies and in councils. Governments and politicians say that until the medical association supports it it’s not validated. In The Netherlands and in Belgium, legislation got up because it had the support of medical associations in those countries. Similarly in Oregon; the Oregon Medical Association at least took a neutral position. And so that’s an important part of why governments or politicians don’t support legislation – it’s not validated at the highest level. Not that I think the AMA is the highest level, but it’s seen as the peer organisation. It isn’t; it represents less than 40 per cent of doctors.
MS: But that would give the politicians some cover?
RS: It would.
MS: Do you expect the AMA to evolve on this issue?
RS: I know there are significant people within the AMA who do support change, but I think it will happen gradually. That’s all I can say.
MS: Can we broaden it a little bit here and talk about death per se? Do you think we talk enough about death in life and in our communities?
RS: No, we don’t. And we ought to. It’s not morbid to talk about death. It’s something that’s going to happen to all us. Because we don’t talk about it, what happens is that thousands of people die unnecessarily protracted and bad deaths – because they simply have not taken the trouble to indicate how they wanted to die.
It is possible under the law in Victoria to appoint a Medically Enduring Power of Attorney, somebody you can authorise to make decisions if you can’t make them. It is possible, not under the black-letter law, but under precedent, to create an advance directive, in which you set out how you want to be treated if you can’t make decisions.
MS: Up to and including medically assisted death?
RS: No. Including the withdrawal of treatment – not prolonging life under certain circumstances. And people ought to realise that the default position if there’s nobody to say `I don’t want the treatment’, you will get the treatment.
That is why we have people’s lives being prolonged by medical treatment in quite ridiculous and unwanted circumstances. Very interesting statistic: a study of doctors’ attitudes showed that in regards to end of life decisions, 40 per cent of doctors provided treatment to patients which they wouldn’t have themselves. Forty per cent. Why? Because there was nobody to say `no, don’t give it’. So the doctor gives it because he doesn’t want somebody to say `you should have done this’ or `you should have done that’. Doctors are frightened of complaint.
MS: Should doctors there Rodney be more proactive in this and say to their patients at an earlier stage of life when nothing’s wrong necessarily `are you aware that you can specify what you want and what you don’t want’.
RS: Absolutely. Absolutely.
MS: So how can we get that happening?
RS: Well again, I think the AMA has a big role to play here. The Health Department has a big role to play in trying to educate doctors to have these conversations. After all, it’s well acknowledged that if you know what your patient wants at the end of life, managing their problem is infinitely easier.
MS: Does this come back to us not, perhaps for reasons of collective cognitive dissonance, not discussing what death means for how you live your life; not only how you die, but how you actually live your life?
RS: I think it does. I do a lot of workshops and counselling and time and again people say `I’ve tried to talk to my children about this but they say don’t be morbid, we don’t want to talk about it’. And I say ``well you’ve got to thump the table and make your children listen to what you want’.
There is this reluctance to talk about it. There shouldn’t be. I think there’s a fear of death, not so much a fear of death but a fear of dying, and how we’re going to die.
I don’t fear death at all. It could happen tonight and that would be that. My experience in medicine absolutely leads me to the view that when we die, that’s it. Ashes to ashes, dust to dust. I think a lot of this fear comes from the old idea of a life after death and people are frightened as to how they’re going to be judged and this sort of nonsense.
MS: It brings to mind a certain Shakespearean soliloquy – we’ve been examining this for a long time, haven’t we?
RS: Confronting that final question.
MS: Well, what would you say to somebody who opposes medically assisted death with dignity on religious grounds?
RS: I’d say that’s fine. I don’t mind. You can believe that. You can go to your death with intense suffering or you can allow your god if you think to make the decision, but please don’t impose that on me or anybody else who doesn’t want that. And that’s essentially what is happening today.
Because our laws have developed out of canon law – we go right back to the Middle Ages. And the law very much reflected what the church believed. They have this term `natural law’, which sends shivers down my spine. Much of our law is derived from canon law and this has got a religious basis to it and it’s very slow to change and the whole tenor of the last three or four hundred years, with the development on the Enlightenment, which to me has given me my values in life, is that the individual has a fundamental value, and that’s the one I respect.
So, if I have a patient who is asking me rationally for assistance, my conscience tells me that I should listen to that very, very seriously. And I do – despite what the law says.
MS: You talk, Rodney, of existential suffering on top of the evident physical and psychological pain associated with the end of many people’s lives. Can you expand a little bit, please, on that idea of existential suffering?
RS: Well, to some people it’s a difficult concept. The word existential, and existentialism, which grew out of Jean-Paul Sartre, I think, is a very dense sort of philosophical concept but it derives from the word existence, which is how you are, how you are at the present time.
And there’s no doubt in my mind that in some circumstances, a person’s existence can be intolerable. Suffering is loss. When we lose things, we suffer. If you lose money at the races, you suffer, but in a much more specific sense. If you lose physical attributes, you are suffering. And the greatest thing you can lose, to me, is your mind. And therefore I look at the person with dementia as having the most extraordinary existential suffering. Now, many people say ‘oh, these people are not suffering, they can’t be suffering, they can feel anything’.
I reject that utterly. I think not only do they suffer great physical suffering that is not recognised because they can’t express it. I’ve witnessed a person in terminal stage dementia over a continuous four-hour period and recognised an enormous degree of physical suffering that was not being recognised or relieved. But there’s (also) existential suffering. If you sitting there could look into the future and see yourself in end-stage dementia, would you not recoil in horror and say that’s not an existence that I want.
There is suffering in the loss of everything that means anything to you. And the suffering that is inflicted upon your family as a result of that is enormous. And their suffering in your suffering. So I think we take a very limited view of suffering. Most people don’t think about it.
There’s a wonderful essay, which I refer to in my book, by Eric Cassell, a medical physician and philosopher. He talks about the nature of suffering, and I may be misquoting, but I think he says something to the effect that suffering is not of the body but of the whole person. And the whole person in includes the mind, so this is why I also believe that people van have the most extreme suffering from mental disturbance. There are people with schizophrenia and untreatable chronic depression who have the most appalling suffering.
MS: I was just about to bring mental health into it, Rodney, because, for example in that case you cite, chronic extreme depression - which is not an uncommon thing and then you the very common situation of people who go through bouts of profound depression. How do you factor that in, and going back to your earlier comments about safeguard caveats, how do assess whether that is something is symptomatic of a situation at the time or something that reflects profound inconsolable suffering?
RS: This where you need – and I talked earlier of it – the dialogue. These are questions that a doctor has to address. It is absolutely true that some people with minimal physical suffering will have an extreme psychological reaction which makes them request assistance to die.
The shock of being told they’ve got cancer may be enough to generate a request but of course that needs treatment of their psychological shock and persuasion that they should entertain treatment. Many people who are at the end of their life will have a depressed move because of their circumstances. A/ they know they’re dying. B/ they’re suffering intolerably. And of course they’re not going to be jumping over the moon. But that’s not clinical depression. That’s a rational reaction to their circumstances and so you can define these matters.
On the other hand you’ve got the person who truly does have just primarily a psychological disturbance. Now, some of those people commit suicide, because in their disturbed state of mind they can’t see any way out. There is a way out, and that is through treatment which brings them through the depression to an understanding that there are other options. And so this is one of the matters that has to be always considered, but I object vehemently to the idea that all people at the end of life who think they might want to die are depressed.
And secondly I object vehemently to the use of the word suicide in relation to these people. They are not committing suicide in the sense that the normal word is examined. They are taking a rational decision. Most suicide - in the terms that it is generally thought of – we are talking of an irrational act. Not that it’s not rational to the person who’s taking their life, but it’s irrational to those who are observing it.
MS: So, in other words these grey areas exist but do not prelude the ability to make decisions about dying with dignity. On the contrary, they compel it, and I’m interested that you use the word – and this goes back to your embrace of The Enlightenment as something very important to you – the idea of rational reactions to circumstance…
RS: I do believe this – that is we are to have legislation that there needs to be, and if I were a politician I would say `right we’ll have this law but before let it loose on the public we will need a very strenuous education campaign of the medical profession’. I don’t think most of them have thought about this issue in particular depth and they would need education as to how the law is to work, what are the issues they need to be careful of.
They’ve done this in The Netherlands; they have set up committees of experts to guide doctors and assist them in decision making, and I would not for a moment try to argue that if law were passed there is not the possibility of error taking place. So it would behove the parliament to ensure there was a proper education campaign for doctors to make sure they understand properly how to implement law.
MS: We’re really getting short of time and I want to sort of move on to you a little bit in terms of how you’ve arrived at this position. Perhaps a good way of doing that Rodney is to look at a couple of case studies that you are aware of – you’ve written a book that looks into a number of cases – to explain and to help people understand how you’ve come to your position.
RS: I’d led a really protected medical existence as a specialist urologist. My patients die, of course, but I wasn’t looking after them. I had this woman with cancer in her spine, cancer from the kidney. She was in my care. I had the responsibility of looking after her and she had the most appalling pain – what’s called neuropathic pain.
It’s nerve stimulation, like when the dentist hits a nerve in your tooth without an anaesthetic. And I got all the resources I could to try to relive this but it was impossible. You need to be under an anaesthetic to not have that pain. And she set me thinking about the realities of this and I knew myself that if I’d been in her position, I would have ended my life. As a doctor, that would have been easy. I’d have had the drugs, the knowledge. But she couldn’t. That struck me as being unfair. I could have said `well I’m alright Jack’, but I thought no, that shouldn’t be.
People in that circumstance should be able to get help. So that was the case that started me thinking about this. And the more and more I thought about it, the more it was like I’d been bitten by a virus, I just couldn’t get it out of my system. It just drove me. I worked out my own position long before I ever read any of the philosophical dialogue. Then I got into the palliative care literature.
Another person who influenced my thinking greatly was a woman in the book who had motor neurone disease, a most appalling aggressive paralysing disease which ends up preventing people from breathing and swallowing and talking and she asked for my help. She was extremely distraught and what I learned from her was that if you entered into a dialogue, an honest, open dialogue with these people, they just said `it’s just terrific to be able to talk to somebody about how I feel’.
And supporting her and giving her medication just had the most profound effect on her remaining life. And I realised the palliative value of having this dialogue and giving people control. I then struggled for years with this sort of fear. I was interrogated by the police over that because I had written to her and I had actually given her some medication – anti-nausea tablets so she wouldn’t vomit when she took other medication. I finally reached a compelling conclusion when another man with motor neurone disease, which I describe in the book, he wanted to assistance and for the first time I provided somebody with barbiturates, which are the ultimate medication, if you like, because if you take a dose of barbiturates of appropriate nature, you just go to sleep in the most beautiful, peaceful, calm manner, and don’t wake up and die relatively quickly.
And I did that for him and he died in the bosom of his family. You know, we talk about birth rite. I think we should consider more about a death rite, or a last rite. I think everybody should have the right to die in the company of their family, in peace and dignity and security. We don’t have that at present. People are frightened of being with their loved ones when they might want to hasten their death because they think they’ll be prosecuted for assisting. I mean, we’re so unkind to ourselves. This is word that Pamela Bone used, wonderful lady, we should be more kind to ourselves and we’re not. We make death into something that can be terribly brutal and harsh. It saddens me, frankly, that we can’t be more mature in our debate about this matter.
MS: We could talk for hours about this, and I’d love to, from a lot of angles, but we can’t. What’s the hardest thing that you’ve had to do?
RS: I think the hardest thing was writing this book.
MS: Why?
RS: Well, I had to really expose myself on a number of levels. Despite what you might think as I’m talking openly about these things, I’m actually a very reticent, shy person. I’ve become much more open as I’ve got older, and I thank, particularly, my wife for that. She’s taught me an enormous amount about understanding emotion becoming a more sensitive person. But it really was an epiphany, a catharsis an exposure of myself, which wasn’t really what I wanted to do.
I wanted to just tell these stories so that people would have an understanding of the context within which these decisions are made. But as I was central to every story, I couldn’t do it without exposing myself, but also exposing what I was doing. And essentially some people would say that what I’m doing is breaking the law. And so that was sort of threatening.
And as I wrote each story I would sort of have a look at myself and say goddammit what are you bloody doing here? You’re an idiot. And then I’d say no, I think this is something that has to be done and so I just kept going. And I’m proud of this book. I think it’s a good book, and I think if people read it they will earn a lot about death and dying and they may learn something about themselves if they think about the stories.
MS: Rodney, I just want to thank you for your time and I want to thank you for helping to lead in our community on something so important. Thank you.
RS: Thank you for the opportunity.
Letters in The Age on 8 February 2011 in response to the above item:
I AM a 68-year-old psychologist. Three months ago I received a diagnosis of Alzheimer's disease. I have been in a state of turmoil, confronted with the existential reality of death.
I have had to take the advice of competent professionals, including my wife, who is also a psychologist, while I prepare for developing mental incompetence and, finally, death. At first I was agitated and anxious. I am now able to think rationally about the uncertainties I face. The change has occurred because of the loving acceptance from my wife, family, close friends and colleagues.
I want to die with dignity. I want to have a part in the decision to end my life and I do not want to be a burden to others as I become progressively incompetent.
I am aware of those who might regard my claims about being a burden as not being wholly valid. I can even imagine some who would regard what I consider a burden to be an opportunity. I think that such re-framing is disrespectful.
I am grateful that people such as Rodney Syme (The Zone, 7/2) exist. I hope that my ending will be responded to by people like him. In this regard, I know I can count on my wife's love for me.
George Wills, Mount DandenongDR RODNEY Syme raises the most important question for anyone under medical care at the end of life: why does patient autonomy stop when they're dying? Why does a police officer have to arrest a doctor because of treatment requested by a competent patient?
Laws should protect a person's integrity from being violated, not interfere in matters where patients and doctors agree on medical care. Neither the government nor the police should be peering under the bedclothes of the dying.
Palliative care is care for the dying, for whom the primary goal is quality of life. It doesn't, and shouldn't, involve misapplied and unenforceable laws that cause prolonged suffering for those requesting relief.
Janine Truter, The BasinLetters in The Age newspaper:
THANK you, Dr Rodney Syme, for your courage and dedication (The Zone, 7/2). Many Australian opponents of physician-assisted dying (a more accurate term than voluntary euthanasia) make misleading statements about what happens in other places where dying with dignity legislation has been enacted.
According to the Oregon Public Health Division's 2010 annual report, 65 known deaths occurred last year from ingesting medications prescribed under the Death with Dignity Act (drugs issued to terminally ill patients only after thorough assessment, and the patients were sent home to use them at a time and place of their choosing).
This corresponded to approximately 21 such deaths per 10,000 total deaths in Oregon. Since the law was passed in 1997, a mere 525 patients have died using its provisions.
I do not find these statistics disquieting. It is human nature to fight for life until life is no longer bearable, at which point compassionate assistance should be our right.
Anne Riddell, MelbourneRE ''LAST rights'' (The Zone, 7/2). There is enough medical and legal information to show that the laws in those countries and states where euthanasia or physician-assisted suicide have been legalised are fraught with problems and deficits.
When is The Age going to be brave enough to publish the other side of the euthanasia debate?
Anne Smith, BuxtonAnti-euthanasia and pro-euthanasia letters – Victorian Senior February 2011
Neil Francis (Seeking law on assisted dying, The Senior, December 2010) peddles “the will of the people” argument that the majority of Australians support euthanasia as something of a fait accompli.
Repeat something often enough and people will always assume it’s true.
But the polls claimed and repeated ad nauseam that something like 85 per cent of Australians support euthanasia law are based on a question that does not reflect euthanasia as it is practised anywhere in the world and bears no relationship to any particular legislative framework.
All that can be said accurately is that 85 per cent of Australians agree with the polling question.
Through all this, Mr Francis, like so many of his colleagues, masks the reality that we’re really talking about doctors killing people by using softly-softly terms like ‘aid-in-dying’, and in doing so paints himself as some sort of modern-day Florence Nightingale.
I urge your readers to take the time to find out what really happens in a modern palliative care environment.
Make judgements based on reality and not scaremongering.
Paul Russell, director,Dying With Dignity spokesperson Neil Francis sends an unhealthy negative and pessimistic message to the community.
To encourage and assist others, particularly the sick and elderly, to take their own lives can’t possibly be reform, but rather the entrenchment of a pattern of despair.
There is no dignity in suicide, whether assisted or self-inflicted.
Claims of “choice and dignity” are utterly misleading since many people who deep down do not wish to end their lives are made to feel a burden on their families and society.
They receive hardly any encouragement to resort to palliative care – the positive antidote for and alternative to euthanasia.
What example does all this set for young Australians among whom the suicide rate has accelerated in recent decades?
Australia does not need laws promoting death.
We need laws that assist all our citizens, young and old, to live their lives, with all the positive facilities available, in such a way as to preserve their true human dignity, not deny or undermine it.
Peter Phillips, SpringvaleIn nature the sick, diseased and crippled are eliminated for the benefit of any one species as a whole.
In other words, the health of the whole is more important than the individual, to maintain balance.
We don’t see nature out of balance, but the human community is.
Humans are the only species that inflicts misery and suffering upon its own by incarcerating the terminally ill into medical facilities that keep them alive as long as possible, thereby inflicting maximum misery and suffering to the individual.
We euthanase a dog when it cannot hold its bladder or is blind with old age, saying that it is humane and the right thing to do.
If it is the right thing to do to euthanase the dog, why is it not the right thing to euthanase a human?
Instead, we inflict suffering and misery on our own for the sake of some medical, religious or politically correct point of view.
It’s time these people thought of others instead of themselves and listened to the cries of suffering.
My body is terminally ill with no hope of recovery. I don’t want to be remembered by my family as a suicide statistic.
I want the right to die humanly, just like the dog.
PB, Name and address supplied.Euthanasia letter from The Senior, March 2011
Isn’t it wonderful that those who continue to find such fulfilment and joy in living are so willing to insist that life must be maintained in all people (Will of the people not so strong, from Paul Russell and Peter Phillips, Your Say, February).
Have these people given thought to the fact that others who desire an assisted death have also lived, loved, laughed, hoped and grieved, and have now determined – for themselves only of course – that hope no longer ‘springs eternal’ and the desire to continue this life has faded and gone?
Such decisions have not been made lightly, nor quickly.
Money cannot buy happiness and ‘hope’ cannot be provided where hope is no longer to be found. And who is to say there is no dignity in suicide? There is no greater dignity than having the personal choice to continue to live, or die, with equanimity of spirit.
I make no effort to deny either of these gentleman the right to voice their personal opinions and/or beliefs; but how dare they undertake to speak on my behalf, or on behalf of other people.
Euthanasia must become the legal ‘choice’ of each and every person.
Why should some people be forced to continue to live a miserable life to appease those who have never had to walk in their shoes and so cannot begin to understand the reasons why life has become so unbearable?
Nola Martin, Preston.Letters in the Victorian Senior April 2011
THREE letters in The Senior’s February issue dealt with euthanasia.
The first two made it clear they had not walked this path, either personally or with a beloved older relative. Neither have spent years visiting a hostel or a nursing home.
If they had, they would know there is very little human dignity left in the lives of our elderly, however gentle and humane the dedicated staff are.
I have sat with people, still of sound mind and not depressed, simply saying “enough is enough, I am waiting to die and I would like just to go to sleep knowing my passing will be painless”.
There is no dignity in dribbling down your shirt front, in not being able to shower yourself, not having control of your life after 80-plus years.
There certainly is no dignity in incontinence, even if the incontinence industry invents a new product every week.
Civilisation has consistently evolved towards greater humanity. We have not perfected it but this has always been the goal. There is no question of people being bullied into dying; simply that those of sound mind, who have made this decision, should be able to carry it through.
This is not a negative attitude. It gives us power and removes the fear that most of us have about how we will die.
Palliative care is simply a much slower course to death.
I Jones, Heathcote.I am one of the 85 per cent of people who favour euthanasia.
I am sure Florence Nightingale was aware of it in the Crimea.
I wish I had met one of those doctors who use the softly-softly method when my father was dying a slow death.
The people who advocate euthanasia are not scaremongering; they are providing a sevice to the sick and dying.
I feel sorry that Paul Russell (Your Say February 2011) is so nauseated by the number of people who want to have this choice.
I hope that I can find a doctor, if I need one, to assist me in my departure from this world to put an end to my misery to help my family.
That’s humane; that’s reality; it’s also an educated choice.
Eileen Lindsay-Stewart, TraralgonLINKS
Red Jos: HUMAN RIGHTS ACTIVISM
Mannie and Kendall Present: LESBIAN AND GAY SOLIDARITY ACTIVISMS
Mannie's weblogs may be accessed directly by clicking on to the following links
Activist Kicks Backs - Blognow archive re-housed - 2005-2009
RED JOS BLOGSPOT (From January 2009 onwards)
This page was created on 12 JANUARY 2011 and updated on 7 JULY 2021