

Article from The Age:
By Benjamin PreissSupporters of voluntary euthanasia have applauded a decision for a state parliamentary inquiry to investigate "end of life choices".
Voluntary euthanasia is likely to be explored in detail by the inquiry, which will report back by May next year.
Greens MP Colleen Hartland said voluntary euthanasia had been taking place "in the dark".
"There are doctors out there assisting people to die," she said. "I'm hoping there will be several doctors that will give evidence about what they've done."
Ms Hartland, who supports voluntary euthanasia, said she hoped doctor and euthanasia advocate Rodney Syme would also give evidence.
On Thursday the Victorian upper house voted in favour of an inquiry by the legal and social issues committee.
Sex Party MP Fiona Patten, who has campaigned in favour of voluntary euthanasia, said the inquiry would determine what legislation was appropriate for Victoria.
"This historic move is one step closer to recognising community support for a right to a dignified death," she said. The Voluntary Euthanasia Party also welcomed the move.
The inquiry will consider palliative care and the need for laws to allow citizens to make informed choices for managing their end of life.
A spokeswoman for Health Minister Jill Hennessy said: "This is a very complex area and it's important that a parliamentary committee look at this issue closely," she said.
Article from WA Today:
By Rodney SymeProvoking the law is the only way to secure change to lift the uncertainty doctors face when making decisions relating to death.

Lethal drugs used for voluntary euthanasia.
It is a self-evident truth that dying can be accompanied by intolerable and unrelievable suffering which may escalate as death approaches. It is also self-evident that some suffering will end only with death. Doctors have an ethical duty to relieve suffering, and to respect the autonomy of their patients. The Medical Treatment Act says it is desirable that dying patients receive maximum relief of pain and suffering. So what does a doctor do when a person with intolerable and unrelievable suffering asks for assistance to die to relieve that suffering?
Such a doctor must operate within a legal framework of uncertainty. The Crimes Act says it is murder to intentionally end a life, even if a person is dying, even if only by a few hours. It is manslaughter if one can foresee that an action will cause or hasten death, and still take that action, and there is a further relevant offence of inciting, or aiding and abetting suicide. A doctor treating people at the end of life can come into potential, and actual, conflict with all these laws, which carry substantial penalties. What should a doctor do if his conscience tells him he should provide relief from that suffering, if asked by a competent patient? Should he hasten death and risk the impact of the law?
I have, for reasons of conscience and perverse nature, been challenging the law surrounding end-of-life decisions and actions for nearly 20 years.
Doctors have been facing this dilemma for centuries, with no protection from the law, and have had to help their patients secretively, or travel under the umbrella of intention, a vague and uncertain defence. More than a century ago, Sir William Osler, a doyen of modern physicians, said "it was the duty of physicians to ease death". And they have done so, with the sword of Damocles hanging over their heads, which is why medical assistance at the end of life is hidden, and so arbitrary in nature. It depends on who you are, whom you know, what disease you have, and where you are living, but most importantly, on the courage or fear, and moral views, of your doctor.
I have, for reasons of conscience and perverse nature, been challenging the law surrounding end-of-life decisions and actions for nearly 20 years. In 1996 I first became aware of the practice of terminal sedation, also known as deep continuous sedation, whereby dying persons, in palliative care, were put slowly but progressively into a coma, without the provision of hydration, and maintained in that state until their clearly foreseen death � and such deaths were not reported to the coroner! They were clearly the result of an anaesthetic process, and could hardly be considered "natural deaths". It took four years, and three deaths influenced by terminal sedation, managed by me and reported to the coroner, before he confirmed that such deaths were not reportable.
In 2005 I gave advice and medication to Steve Guest, who was dying of oesophageal cancer. He took this medication to end his suffering, and over the next three years I made statements which a drover's dog would understand about my involvement with his death. In 2008, my book A Good Death was published by MUP; in that book I described my involvement with 20 of my patients and of my assistance in their deaths, including that of Steve Guest.
Two police interviews followed, but no action. Realising that the police could reasonably argue that they did not have sufficient evidence to prosecute me, I finally acknowledged a year ago that I had given Nembutal to Steve, but also argued that my intention was to palliate him by giving him control over the end of his life and improve his quality of life. There is ample evidence that it did so. A further police interview followed, but no prosecution, on the grounds that "there was insufficient evidence". It is not clear whether a referral of the matter was made to the Office of Public Prosecutions, because only silence has followed.
Since then, I have provided advice and medication to another 10 people, including Peter Short. Brave Peter did not take this medication, dying well in palliative care. Nevertheless, it provided him with powerful palliation. His medication has rolled over to Ray Godbold, a palliative care nurse dying, by strange coincidence, of the same oesophageal cancer as Steve and Peter. Ray is acutely aware of the reality of dying in palliative care, and wants another palliative option. It is not my intention that he end his own life, and I hope he does not need to, but having that choice is powerful medicine. It is an alternative to terminal sedation.
The Office of Public Prosecutions is between a rock and a hard place. It regularly prosecutes laypeople who are involved in the deaths of suffering relatives, regrettably because they have felt they had no alternative. Our judges show their dissent by regularly finding no reason for punishment in these cases. Law Professor Loane Skene says doctors are extremely unlikely to be prosecuted on the ground that it is not in the public interest � a jury would be highly unlikely to find them guilty of a clearly merciful act, and furthermore, such a prosecution would have a disastrous effect on the future palliation of suffering patients.
It is gratifying that the Victorian Parliament has at last established a parliamentary committee of inquiry to look thoroughly into this matter.
My journey has been one of provoking the law, or more specifically, the lack of law in relation to necessary medical actions at the end of life. We proudly say about our democracy that we live by the rule of law, but as a doctor, I find an absence of clear end-of-life law has a profound effect on doctors, their patients and their families. I grieve that this status quo exists despite clear logic for change. Such a status may need a shove for it to change � that is what I am hoping to do. Sometimes non-violent civil disobedience is that shove.
Dr Rodney Syme is a former vice-president of Dying with Dignity Victoria.Letter The Age 15 May 2015"
Dr Rodney Syme speaks of "non- violent civil disobedience" ("Disobedience: a path to clarity in end-of-life law", Comment, 14/5). How brave of him to risk his freedom to help the rest of us die a little more comfortably. Death is one thing that every person has in common. It will come to us all. Once you have watched someone die, especially a loved one, the matter is suddenly strongly in focus for each of us. Those of us who want a choice at the end of our lives do not want to make choices for for anyone else � just ourselves. Dr Syme, you are a wonder, someone who wants to help, not for your own gain, and knowing there is little glory in it.
Sally Dobson, South Melbourne
Euthanasia Letters in The Age:
I admire Rodney Syme's courageous and considered position on end-of-life law ("Disobedience: a path to clarity in end-of-life law", Comment, 14/5), but I have serious doubts that the clarity he seeks is achievable by trying to provoke his prosecution. As his cited case of the late Peter Short exemplifies, many passionate advocates for euthanasia die peacefully in palliative care, having gained enormous comfort by knowing that Dr Syme was "in their corner", ready to assist in providing them with a speedy exit if they became convinced their alternatives were intolerable.
As a 30-year oncologist, I have observed numerous patients and their family members benefiting from the quiet bonding and connection that often occurs around the bed of a dying patient in the final days. Doctors are already protected by the principle of "double effect" in relieving terminal suffering, and the research about how to provide a comfortable death is progressing rapidly. I believe advanced care plans are more important than developing detailed right-to-die laws. Sometimes the best outcomes are achieved by leaving difficult moral decisions in a grey area for sensible, wise and committed people to work in.
Ian Haines, Hawthorn EastHow I admire Dr Syme, a man who will put his comfort on the line in order to help those who wish to be able to decide how to cope with pain and mental anguish. Nearly 15 years ago he gave my husband and me counsel, but it would have meant moving him from St Vincent's, where he was dying. We took the oncologist's reluctant advice to hasten the end by removing nephrectomy tubes, denying fluids and dispensing more morphine. It turned out a cruel way to leave this world. When will the people who speak on our behalf have the courage to let us decide for ourselves, when the end is painfully inevitable? My letter regarding Gordon's death was published in January, 2001. Nearly 15 years on and still, despite at least 80 per cent of the community wanting choice, not much has changed.
Anna Sewards, Mitcham
Dr Syme sees giving Nembutal to patients as a "powerful palliation" tool, giving them control. I wonder if conversations that truly explored his patients' deeper underlying vulnerabilities, fears and need for control had been held. Had specialist holistic palliative care been given? Is he robbing the person and their loved ones of the opportunity for further healing even at this final stage of life? Palliative care physicians have pleaded for funding for research, training and education before allocating resources towards legalising euthanasia. Dutch ethicist Theo Boer once supported euthanasia but now, having seen its effects, advocates against it. It is imperative we listen to these voices.
Carol Ong, East MelbourneIt is all very well for people who have the capability to decide they wish to die, but what about the incapacitated in nursing homes? They have no voice. Every day they are hoisted out of bed, stripped, washed, dressed and nappied, then hoisted back into bed or into their conveyance for the day. They may be fed and looked after well, but they can't walk, talk or scratch themselves. The only benefit in keeping them alive is to keep people employed. Three shifts of nurses, carers, cleaners and kitchen staff, 365 days a year. Then there is work for chemists, doctors, nappy manufacturers, food suppliers and so on. This has been my husband's life for more than three years. If he were a dog we could be more compassionate.
Kerrin Adams, Glen Iris

Cancer sufferer Ray Godbold, left, talking to Dr Rodney Syme, of Dying with Dignity Victoria. Photo: Justin McManus
Doctors, politicians and lawyers have come out swinging after a controversial urologist saw his invitation to speak at a prestigious national medical event rescinded.
Dr Rodney Syme was set to headline a plenary session and "end of life" panel discussion at the annual conference of the Royal Australasian College of Physicians later this month, but has been "uninvited" from the Cairns event. Fairfax Media revealed last week that Dr Syme publicly handed lethal illegal medication to a terminal cancer victim, Mr Ray Godbold of Inverloch. The exchange of the drug Nembutal � commonly used by vets to euthanise pets � was an act of defiance meant to draw attention to the "right to die" issue.
Dr Syme said the retracted invitation exposed "astonishing rudeness" from the college on one level and "amazing cowardice" on another.
"It's an issue of academic censorship," Dr Syme said, "and an example of the length and depth to which those ideologues who are opposed to this issue will go, in order to suppress the conversation."
The RACP said through a spokesperson that Dr Syme had been uninvited prior to the publication of his most recent action. They added that the situation was "regrettable" and the decision � made after "careful consideration" � was "a difficult one, but it accurately reflected the membership's feedback."
The move has drawn the ire of many, however, including former chief minister of the Northern Territory, Marshall Perron, who wrote to the RACP to lambast their "disgraceful" action.
"As a supposedly professional body the organisation should encourage open honest discussion on issues of great interest to our ageing citizens," he wrote. "Instead you demonstrate a cowardly approach of which you should be ashamed."
Sydney GP Dr George Quittner also wrote to the college, appalled that Dr Syme had been "gagged". He urged the college to reconsider their "damaging" stance.
"Doctors who stand for honesty and integrity in their clinical work as well as their personal philosophy will reject you and your college for this cowardly and shameful act," he wrote. "It is not in the spirit of our profession, or the Australian commitment to freedom of expression."
Melbourne barrister Julian Burnside, a patron of Dying with Dignity Victoria for more than a decade, said the action was "interesting and disappointing" � but not surprising.
"I fear that the Australian appetite for free discussion of ideas is diminishing," he said. "We seem to be much more comfortable hearing opinions we agree with than those that challenge our view of the world."
It has been a week since Dr Syme and Mr Godbold allowed their consultation to be chronicled, and yet neither man has so far been questioned or charged by Victoria Police.
In Victoria it is a criminal offence to incite, aid or abet a suicide, with a maximum penalty of five years' jail.
Nembutal is also a "border controlled drug", possession of which is a breach of law with penalties including imprisonment or fines of up to $825,000.
Mr Burnside said he was pleased that Victoria Police have not yet moved on the men.
"I'm impressed that they haven't, because an immediate knee jerk reaction would be to jump in and raise a flag to say you're cracking down on this kind of thing," he said. "Instead they've shown restraint and common decency." Dr Syme, the vice-president of Dying with Dignity Victoria, has been investigated in the past regarding previous admissions of supplying Nembutal to terminally-ill patients, but has never been charged.
A spokesperson for Victoria Police said that they will not provide running commentary on any investigations.
"I don't expect that there's very much they can do," Dr Syme added. "And if in the fullness of time there is no action, the less clear the law becomes and the more confident doctors can be in providing their patients with what I believe is good palliative care."
Euthanasia Letter in The Age:
My heart breaks a little. How I respect Ian Haines (Letters, 16/5) and Rodney Syme (Comment, 14/5). Both made extraordinary contributions to the life and death of my husband Peter. Ian by way of his extraordinary care of Pete since his cancer diagnosis in 2008. Ian's commitment to his patients is humbling. In 2014, Rod, too, gave Peter care and considered advice. He also gave him Nembutal, Peter's lifeline. This enabled peace of mind and took away fear around the process of dying.
Both played significant roles in the palliative process. But this should not be an "either/or" debate. Choice at end of life should be part of the palliation package. That would allow, as Ian says, "quiet bonding and connection around the bed of a dying patient", and the ultimate decision made by that same patient and their family, not medical professionals, no matter how sensible, wise and committed.
Elizabeth Short, CamberwellThe Age euthanasia letter:
True compassion is not only expressed through assisting dying people to "contain and tolerate their feelings of distress, fear, abandonment, helplessness and pain" ("Euthanasia is not merciful: there is meaning in life in even the deepest pain", Comment, 20/5). Human dignity is intrinsic and generally understood as treating each person as worthy of honour and respect in their own right.
Hopelessly ill and dying patients want to be listened to � but also heard. This means affording them respect by not thwarting their wishes, or treating them as mere means to ideological or religious ends. Offering formal and informal support to people as they work through difficult life decisions that may differ from one's own can be challenging, especially to those holding entrenched views against choice for voluntary euthanasia.
Like many such opponents, Mary Ticinovic cites the Hippocratic oath; or the injunction to "do no harm". Hippocrates was born in 460BC, before any medical profession as we know it. (The oath begins by swearing to Apollo and all the gods and goddesses.) Oaths required by medical schools today vary from none to edited statements revealing historical origins. Incurably ill patients with unremitting suffering may decide, after consultation, that a peaceful death offers them the lesser harm. To deny them this choice is callous, disrespectful and undermines their dignity.
Julia Anaf, Norwood, SAArticle in the Sunday Age:
Broad support will let community have a say on care and laws for people to make informed decisions about life and death.

A bottle of Nembutal can end a life, and many people would like to have one on the table. Photo: Justin McManus
A subtle but significant step towards voluntary euthanasia took place in the Victorian Parliament this month, but chances are you probably missed it.
While most of Spring Street's attention was focused on Daniel Andrews' inaugural budget, the state government initiated an inquiry that maybe � just maybe � could pave the way for a legislative shift in the right to die with dignity.
Two weeks ago, upper house leader Gavin Jennings introduced a motion for a parliamentary committee to "look at the need for laws in Victoria to allow citizens to make informed decisions regarding their own end-of-life choices".
Boiled down, the committee's review would cover three areas: palliative care and the practices used by the medical profession to help people manage their end-of-life treatment; the current and proposed legal framework in Australia and overseas; and what type of legislative change may be required, including the impact of any federal laws.
Jennings' motion was carefully worded and deliberately open-ended in a bid to maximise support within the broad church of the upper house, where the government doesn't have the luxury of a clear majority.
It was also crafted after several discussions with Greens MP Colleen Hartland (who had earlier moved her own motion asking for voluntary euthanasia to be referred to the Law Reform Commission) and the Sex Party's Fiona Patten (who had foreshadowed alternative plans to reignite the debate). Both are largely responsible for pushing the issue forward by bringing it to a head sooner than Labor might have liked.
In a surprise result, the motion passed resoundingly � 29 votes to 9 � not only with the backing of many Coalition MPs, who were allowed to exercise a conscience vote, but also with the support of DLP and the Shooters and Fishers, two of the more socially conservative forces on the crossbench.
What this means is that the community can now have a say on the appropriate models of care and legislation required for people to make informed decisions about life and death.
Public consultation will take place in coming months. Hearings will be scheduled and witnesses called. And the upper house committee conducting the inquiry � comprising three Labor MPs, three Coalition MPs, and one representative each from the Sex Party and the Greens � will have until May next year to finalise its recommendations, which the government must then consider on merit.
Whether this results in voluntary euthanasia being legalised in Victoria remains to be seen, but at least the public has a forum to talk about it. As Jennings said earlier this month: "As complex and vexing as these issues may be, it is incumbent upon a modern parliament that is responsible to the needs of its community to take on these issues and be prepared to engage in an active consideration of them."
In the meantime, the government has promised to undertake two important pieces of work: improvements to palliative care services, including a shift towards a home-based palliative care model; and new laws giving people clearer rights to set directives about the kind of medical care they want � or don't want � in the event of future conditions such as cancer, brain damage or dementia.
At present, people can stipulate what kind of treatment they'll accept when it comes to an existing medical condition, but the guidelines around future illnesses lack clarity. Andrews has been keen to tackle this ever since he was a health minister in the former Brumby government. Now as Premier, he's determined to create a more flexible system.
Voluntary euthanasia, on the other hand, is a much harder issue to tackle, particularly when a large number of state MPs don't support it. Nonetheless, there are several truths the parliament inquiry may be forced to confront.
The first is that despite vast improvements in palliative care, it simply isn't possible for every terminally ill person to die without pain or intolerable suffering.
The second is that many patients who are given the means and knowledge to choose the timing of their own death are helped simply by having that choice because it mitigates their fear and anxiety. Figures suggest only about 30 per cent ultimately choose to end their own lives.
And the third inescapable truth is that in Victoria, euthanasia is happening arbitrarily, whether you like it or not. Some patients simply end their treatment and are given medication to hasten their death; others have doctors who provide the drugs and advice to take their own lives.
Indeed, this month The Age revealed high-profile euthanasia campaigner Dr Rodney Syme had publicly handed the lethal illegal drug, Nembutal, to a terminally-ill cancer victim as an act of defiance designed to draw attention to the issue.
Syme is yet to be approached by police, nor does he expect to be, but his story highlights, yet again, the difficult position doctors find themselves in, given the disconnect between the Medical Treatment Act (which encourages doctors to ensure dying patients receive maximum treatment for pain and suffering) and the Crimes Act (which says it is murder to end a life, even when a person is already dying).
End-of-life treatment is complex issue, but if the committee is adequately resourced, the inquiry is thoughtfully administered, and its findings are taken seriously by the government, such a review could set the template for years to come.
And whatever the outcome, parliament should be commended for having the debate. Seven years ago, when the Greens introduced a private members bill to legalise physician-assisted dying, it was voted down 25 votes to 13.
This time, a broader discussion is on back on the agenda, in effect bringing the community one step closer to a resolution on the right to a dignified death
Article in The Age:
I had to identify myself as a clinician before the end-of-life care team rolled into action to help my dying father. Why is it so hard to be heard?

A patient nearing death often feels alone and distressed in hospital.
Recently I sat by my father's bedside as he died. He was unconscious, in a fog of sedation and painkillers, and I had the privilege of a long goodbye. In the end he had a peaceful death, but my family had to fight for it. Fight the passive resistance to providing care focused on a comfortable death, rather than care focused on cure. Fight the lack of recognition that we could simultaneously love this man, while advocating for care that allowed him to die without agitation and suffering. Fight the insidious guilt this conflict let creep into our last week with him.
In itself this is not a remarkable story, our difficulties navigating the end-of-life landscape have been shared by countless other families. What is remarkable is that our experience was so difficult despite my role as a senior intensive care specialist in the Australian healthcare system, a clinician who regularly deals with grief and dying. I had imagined I would be able to smooth the bumps for my father and family. I was wrong, and there are lessons I have learnt.
At his most vulnerable, my father suffered, and we were treated clumsily. Over 10 days in hospital, he became distressed and frightened, and lost strength and dignity.
I have learnt it can be hard to be heard. My father had fallen in his courtyard, toppling backwards and striking his head on a rock wall. Hard enough to cause a large scalp laceration, a lot of blood on the ground, a small amount of bleeding into his brain, and needing urgent hospital care.
We asked to talk about treatment limitations because this was much more than a fall and a head injury. It was his second fall in a few months, occurring on a backdrop of progressive dementia and physical deterioration that had slowly but relentlessly taken him from us. A shadow that transformed a man with intellect, humour and compassion, to a frail figure grappling for a mental handhold on the world around him, struggling to remember our names and faces. Cruelly, it left him with enough presence to feel alone in hospital, wishing he were home with the woman he had loved for more than half a century.
We wanted to talk about our fear this injury would lead to a more rapid decline in his quality of life, that he would not be able to return home, and that this would be unbearable for him. We wanted to say we didn't want him to receive care that would prolong his life, only to see him die away from home soon after. It is not easy to say these things about someone you love, and when we did we were told he would get full resuscitation, that the doctors involved in his care were not available to talk to us about treatment limitations until the next day, or the day after that. We were not heard.
I have learnt it is easy not to get good end-of-life care. Although there is growing recognition at all levels of the health system that it is better to provide end-of-life care that focuses on people rather than just disease, it is still easy not to die well. It is easy not to know you are in the last part of your life. It is easy not to be asked what you value in life, or to be offered care that puts this first.
At his most vulnerable my father suffered, and we were treated clumsily. Over 10 days in hospital he became progressively more distressed and frightened, and lost strength and dignity. When he developed urinary retention and could not empty his bladder, it took more than 24 hours for a catheter to be inserted, despite his extreme distress. When we asked if he could have night-time sedation for his delirium and agitation, we were told he couldn't because of his brain injury. Yet at night we were called and asked to reassure and comfort him while urgent sedation was organised. When we expressed concerns that he could not eat or swallow, we were told daily a speech pathologist would see him. Almost comically they came for the first time the day his palliative care regime began, ensuring a carton of thickened fluid was delivered to his bedside three times a day while he was unconscious. When we asked, daily, for a referral to a palliative care team, it took more than a week for it to happen.
I have learnt that good end-of-life care is worth fighting for. After a week of anxiety, we flashed briefly into anger and frustration, and then in desperation we pushed back. I did what I had tried to avoid, and identified myself in my professional role. By the end of the day the doctors involved in his care had spoken to me, understood our concerns, and agreed to our requests for care that concentrated on comfort. When the palliative care team arrived they listened to us, and delivered clear, effective comfort care, lifting a burden of anxiety off our shoulders. It did come at a cost. A cost to my father, who suffered when he could have been peaceful. A cost to my family, left to feel guilty for demanding comfort over cure. A cost to me, because the days spent advocating as a doctor could have been spent grieving and saying goodbye as a son.
I have learnt that our healthcare system is full of vulnerable families and caring health professionals. In the final days, weeks, months of life, when a new event tips the scales further against us, there is lot at stake, and patients and families become vulnerable. Even though we had expected a frailty event like Dad's fall for some time, we were shocked by the sudden lurch into the last weeks of life. We struggled with the immediate threat to his life, then the dilemma of curative or comfort care. There are families like us throughout our hospitals, their loved ones deteriorating with diseases that are progressing, frailty that can't be stopped, and like us they become distressed, become the "difficult family". Unless we identify them, and approach them, we can't help them.
Our health professionals care. As a family we spent hours with nurses who gently cared for my father, and engaged with us as the mood demanded. In a hospital environment that is alien, controlled, full of strange smells, noises, and the lurking threat of suffering, they care, laugh, listen, explain and bring humanity back into the room. They make a difference patient-by-patient, family-by-family.
I have learnt we need to do better. Our story is played out continuously, 24 hours a day, in acute hospitals across our country. The script may differ in details, shades and nuances, but always describes the same journey. In a health system that does a remarkable job curing or controlling diseases, returning us to lives we value, the default is set at intervene. To provide better end-of-life care to patients and families, we need to identify them, offer support, listen, and give advice and treatment tailored to their needs. If we don't, only those lucky enough to know the system, know someone, or stumble across a hospital that is really good at this, will be given the choices we all deserve.
Grief is awful, and dying is a process that takes all our attention. We don't need distractions.
Associate Professor Neil Orford is director of Intensive Care at University Hospital Geelong and director of Critical Care Services at St John of God Hospital Geelong.Article in The Saturday Age:


Andrew Denton has resurfaced after being out of the public eye for three years - to talk about dying. Photo: Luis Ascui
Andrew Denton first met Ray Godbold around a year ago. So did I. We each came down to Inverloch, independently, for his story.
Ray was a brilliant palliative care nurse, struck down by terminal gastro-oesophageal cancer. As a medical professional he knew the often nasty and tactile way our lives can end, and as an activist he took a stand by going public in sourcing an illegal drug to hasten his own death and avoid those horrors, if needed.
But Ray was also a man who eventually died in distress, only recently, because he grew too ill to ingest his banned substance and � importantly � no other option exists in this country for people who want a way out of their anguish and despair.

Ray Godbold sourced the illegal drug Nembutal from the controversial Dr Rodney Syme, in case it was needed at the end of his life. Photo: Justin McManus
There are no laws here to protect doctors who might wish to help hasten the end, and so people in pain are left with no rights regarding the end of their life � they are left adrift to deal with their "unbearable suffering".
Unbearable suffering is a term that Denton returned to often this week. He did so in public lectures and on radio and television. After vanishing from Australian media almost three years ago and selling his production company shortly after, one of our most recognisable personalities went into hibernation.
Now finally returned, what does the commentator and comedian want to talk about? Death, apparently.
He wants to talk about the countless accounts of physical and existential suffering that could be avoided here if only we had suitable "assisted dying" laws such as those that exist � and which Denton explored � in places such as Belgium, the Netherlands and Oregon. Ray Godbold is just one man whom such laws could have helped.
"Ray was a gentle man," says Denton, smiling. "Graceful, calm and very chilled. He had his priorities about the world very much in order. He was a funny man. In that position I would be screaming, but he had this quiet sense of humour.
"It was a remarkable, unique thing to spend a number of months with a man who was dying who, because of his skills, can tell you exactly what's happening and knows what lies ahead. I found it difficult."
Ray was dry and upfront. When he slipped on a concrete floor and badly bruised his emaciated frame, he texted Denton with a picture of his injuries and a comment: "You should have seen the other guy. It was Mike," he wrote. "Tyson"
He once told me that if he wasn't already dead right by now, he would be skinny enough to ride in the Melbourne Cup. The only trouble would be looking good in the silks, he said, and choosing the right colours.
Of course funny people can still meet a dark end. Ray dropped his guard occasionally. Denton remembers a quiet interview in which the man admitted he had a brilliant life, a brilliant career, brilliant family, but it was lonely. Dying, that is.
Denton's own father, who used to joke that he would like to die by wading into the deep end of a pool filled with single malt whisky, faced a similar fate 18 years ago when he died slowly of heart disease.
The light left, the happiness faded and the humour went.
"Everything goes, in the end," Denton says. "These stories are being repeated all over Australia all the time. When the topic comes up, I've been struck by how people always � always � have a story about a mother, a brother, father or sister who died badly."
Ray Godbold wanted the right to die with dignity, but was denied his chance by restrictive Australian laws Photo: Justin McManus
"One should always be careful with opinion polls. But the one law of opinion polls is to follow the trend, and the trend in this country is unbroken over many years.
There is no issue on which the public has been more firm in saying what they want than this."
The catalyst for this new body of interviews and arguments in Denton's signature style, however, was not one of the many gruesome tales of death � of lung cancer patients struggling for breath, or people with bowel obstructions tasting fecal matter in the mouth in their final moments.
The inspiration was a positive story he read about the assisted death of a father in Amsterdam � one that followed the strict and formal guidelines developed in other parts of the world to provide people with an escape.
The man spent his final days with family and friends, listening to Mozart, reading an ancient Chinese text and gazing upon the moon before dying at an appointed time, with the assistance of a physician.
"That's civilised. That's humane," says Denton. "Nothing removes the sadness of death, but there are things it is within our power to avoid. And we are looking away from that possibility."
Denton was moved to contact people in these places and understand the process. He talked to the terminally ill but also doctors, academics, lawyers, ethicists, representatives for the elderly and disabled, and people on both sides of the debate.
He travelled all over Australia and the world, recording hundreds upon hundreds of hours of interviews, breaking down the debate and prosecuting the arguments against such laws � arguments that never stood up.
The "slippery slope" tends to be the most misleading of these. Its proponents argue that euthanasia laws could be abused to coerce or devalue the elderly and disabled. Denton investigated countless case studies held up by these lobbies as examples of legislation run wild, only to find the stories had been cynically manipulated to fit a personal ideology.
"I think some people have a deep moral objection to the idea of someone ending their life, and I don't have an objection to that," Denton says. There are also those that believe only god giveth and god taketh away. Holding that view is not wrong. But where they are wrong is when these beliefs are imposed on everybody else."
Using assisted dying in cases of extreme mental illness is another topic Denton seems willing to broach. "Psychiatric euthanasia" might seem anathema to many, but is being navigated in Belgium right now.
Again there are common misunderstandings in play. The laws apply only to people who are legally competent adults, who understand what they are doing. And in many cases, the regimented process of physician consultation and medical panel approval has led to people receiving better diagnoses and treatment, which ultimately saves many lives rather than ending them.
"They are stepping their way through this with great thought," Denton says. "But this part of the issue is very much at the fringes, and focusing on it too much can potentially de-rail the simple premise of relieving suffering."

Andrew Denton has spent several months investigating assisted dying laws abroad. Photo: Luis Ascui
Denton would prefer you consider the bulk of cases we know about, or a subset you may not have considered, such as elderly people who have no terminal illness but a range of ailments that make life agony.
"On average one person per week in this category takes their own life," he says. "It bothers me that we look away from this, when we could be compassionately and rationally addressing a very real issue."
The podcast series he is producing with support from the Wheeler Centre � titled "Better Off Dead" � should be ready by January and potentially sooner, and has been a full-time commitment for several months.
"I wanted to do something that had value. I kept coming back to this subject, and that's the truth for me. I feel there is a great injustice happening here. We're turning our back on people saying we don't hear you, there's nothing here for you."
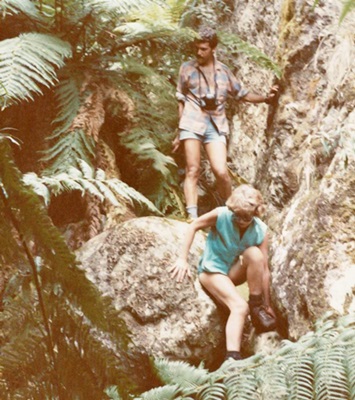
Before taking up this mantle, the Denton career hiatus has not been marked by half-hatched TV program ideas but travel, from Antarctica to the Kimberley � from trekking in the Northern Territory to scuba diving in New Guinea.
"It's what I wanted to do, step out of the office and into life."
He didn't want to produce another show, or host one. "I reached a point and thought, 'I've done this'," he says. "So why would I keep doing this? I know how to do this. Why wouldn't I do something else? I'm really, really glad I did."
"Life," he says, "is the true career".
Seeing the world while he is still young and fit � before he one day becomes infirm and potentially (but hopefully not) faces that unbearable suffering � is all part of his personal philosophy.
Denton has met the dying and those who care for them. He has a sense of what will stay with him on his deathbed.
"Beyond the people I love, none of it will be my work. It's actually going to be those elemental experiences in the wild places of the planet, that are burnt into my soul.
In the career of my life, I consider those to be considerable achievements."
Article in The Saturday Age:

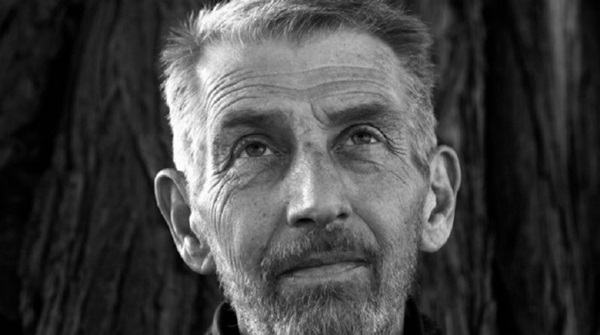
Scientists Pat and Peter Shaw died in a suicide pact in October. Here, their daughters reflect on their parents� plan - and their remarkable lives.

For as long as the blue-eyed Shaw sisters can remember, they knew that their parents planned to one day take their own lives.
It was often a topic of conversation. Patricia and Peter Shaw would discuss with their three daughters their determination to avoid hospitals, nursing homes, palliative care units - any institution that would threaten their independence in old age.
Having watched siblings and elderly friends decline, Pat and Peter spoke of their desire to choose the time and manner of their deaths.
To this end, the Brighton couple became members of Exit International, the pro-euthanasia group run by Philip Nitschke that teaches people peaceful methods to end their own lives.
The family had a good line in black humour. The three sisters recall telephone conversations with their mother in which she would joke about the equipment their father had bought after attending Exit workshops. �He�s in the bedroom testing it,� Pat would quip.
About four years ago, Pat and Peter�s resolve to stay away from hospitals was heightened. While hanging washing in the backyard of their beloved home, Pat, then 83, tripped and broke a bone in her thigh. She was carted off to the emergency department. Her fracture healed well but doctors were concerned about her high blood pressure. They wanted to keep her in and treat it until it was under control.
Pat disagreed. A biochemist who had taught medical students at Monash University for decades, she blamed the medicos for driving up her blood pressure. She said she knew how to treat it and so, against dire warnings, she left the hospital with Peter. Sure enough, when she got home her blood pressure dropped within days.
BELOW Pat with her daughters in the '60s.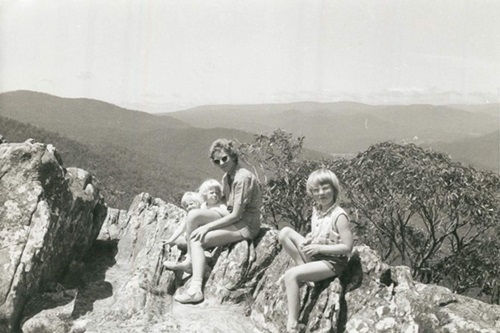

The two scientists relished life. They skied, went bushwalking and climbed mountains, often taking their three young daughters with them. Their cultural and intellectual pursuits were many - classical music, opera, literature, wine, arguments over dinner with their many friends. They donated 10 per cent of their annual income to political and environmental movements. Family events were spent thoroughly debating the topics of the day.
As their capacity declined, the conversation about ending their own lives became more serious and their rejection of what Peter called �religious do-gooders� became more fierce.
�It was also a way into their favourite topics; philosophy, ethics, politics, the law �,� says their youngest daughter, Kate. �The idea that their end-of-life decisions could be interfered with by people with the superstitions of medieval inquisitors astounded them, and alarmed them.�
In April, Peter, an eminent meteorologist, was labouring. He sat down at his computer and typed a letter to his daughters, three highly educated women - two have PhDs and one is a concert violinist in Germany.
�My head swims,� he wrote. �When I am reading, I can�t follow a difficult argument, so I give up, telling myself that it doesn�t matter, and I will read something else. I have just now been reading the history and politics arguments at the end of the latest Quarterly Essay and I am very disappointed that I can�t follow them.�
�My condition is getting worse bit by bit, slowly week by week. On top of all this, my eyesight and hearing are no good, my pulse is occasionally irregular. So how long can it go on? Weeks? Months? As you all know, I am not afraid of dying but I am dead scared of incompetence.�
Pat was also troubled by her old age. Arthritis was corroding her joints and she was getting dizzy, putting her at risk of another fall. She had swollen knees and hands, and was finding it increasingly difficult to get out of bed and out of chairs.
Following Peter�s letter, his daughters tried to keep him and Pat as content as possible. They visited more often. They tried to work out ways of helping. They attempted to cheer up the pair with fine whisky and wines. Surely they wouldn�t go when there was another bottle of duty-free Laphroaig in the pantry, Kate thought.
But her parents had other plans.
Anny, their second daughter, asked if they could wait for one last Christmas. But they couldn�t. Or wouldn�t.
They set a date. Peter said it was time and Pat agreed. They would enter the �big sleep� together on October 27, the day after Pat�s 87th birthday.
Anny got on a plane. When she arrived in Melbourne on October 21, she was shocked at how frail her parents looked. She would often find her father slumped in his chair. Her mother was struggling to move in the purposeful way she used to. Anny showed them a DVD of concerts she had performed with the Munich Radio Orchestra. But she could see that her parents had changed. They were tired. Even a bit bored, she thought.
On their final night together, the family shared a last supper of sorts. The sisters prepared a plate of cheeses, avocado and smoked salmon to eat with wine. Peter and Pat pecked at it. They didn�t seem very interested in food. Anny picked up their grandmother�s violin and played for her parents. They went to bed around 10pm. The next morning, Peter and Pat got up early. They showered, dressed and made their bed. Peter had breakfast, a fried egg and coffee. Pat did not eat. She wanted to keep her stomach empty for what was to come.
The family sat in their backyard in the soft morning sun, enjoying the native garden that had flourished around their Robin Boyd-style home. Peter had designed the house himself in the 1960s.
�They were more cheerful than I had seen them since I arrived,� Anny said.
Everybody knew the plan. The sisters were to leave around noon. They felt they had no choice. Assisting, aiding or abetting a suicide carries a penalty of up to five years� jail in Victoria. Their mother would have liked them to stay, but not at the risk of prosecution.
Pat did not want to die by herself, so she would take a lethal drug first. After leaving her in their bed, Peter would walk alone down the hall of their home and into the living room where they had shared so many hours. He would open the back door and trek one last time through his yard and into his shed where his equipment was set up.
In those final hours, everybody was calm. They discussed the need to lock the doors after the sisters left. People were always coming and going through the house. It would be a bad time for anyone to come knocking.
While Peter discussed the logistics, Pat mused about any final homilies she could offer her daughters before she left them. Peter joked that they had never listened anyway.
�It was all so normal,� says Kate. �I just started laughing at the surreality of it ... and took out my phone to take some photos - something I never do.� And then it was time.
Just before noon, the sisters embraced their mother and father and left. There were no tears.
They walked out of their family home and walked down to the cafe where Peter regularly sipped coffee during his �morning totters� with his friend Frank. They wandered on the beach where they had grown up, and waited.
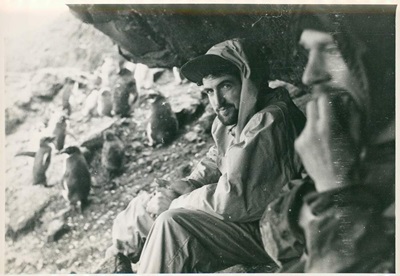
BELOW Peter Shaw (centre) on the Antarctic expedition for which he later received a Polar Medal.
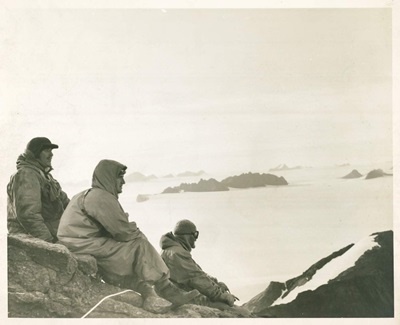
Somewhere in Antarctica, there is a mountain named after Peter Shaw. He conquered it in 1955 on a pioneering mission with the Australian National Antarctic Research Expeditions. The following year, he was awarded a Polar Medal for the mission and he was immortalised on a postage stamp. The trip had been tough. He and his companions had endured at least one terrifying storm that was so traumatic no one ever spoke about it again. They relied on candles for light and layers of wool for warmth. There were no fancy gadgets.
The year that Peter stuck an Australian flag in that peak was the same year he fell in love with his sweetheart.
Patricia was the �it girl� in their mountaineering club. Dazzling blue eyes and blonde hair. But Pat - or Patsy as she was sometimes called - was more comfortable in shorts and hiking boots than dresses and baby-doll heels. She was whip smart, too. Had plenty to say and knew what she was talking about. The first time Peter ever saw Pat, he later told the girls, he had turned to a friend at the club gathering and asked who she was. The attraction was mutual. They married when they were 27.
During the 1950s, Peter worked as a meteorologist for the Bureau of Meteorology while Pat, one of the first women to study biochemistry at the University of Melbourne, worked as a nutritionist. She took a break from it in 1957 to have her first daughter. But she never fancied herself a stay-at-home mum. After their next two girls arrived in 1959 and late 1960, Pat started teaching at Monash University where she became a lecturer in the medical faculty.
In the early 1960s, Peter read the weather for the ABC and Channel Seven - a small taste of fame. But he was no peacock. He was better known for his principles and dedication to the Professional Officers Association where he concentrated on winning fair pay and conditions for his peers. He was admired for his encyclopedic knowledge of meteorology, and for his ability to be direct and frank when something needed to be said.
An old colleague, Michael Hassett, recalls him flooring everybody at a meeting in the late �70s about a controversial plan to collect data on Bureau of Meteorology employees. After several timid questions from the crowd, Peter stood up and said, �I don�t have a question, I want to deliver a tirade.�
�He lambasted the proposal as a thoroughly bad idea from start to finish and suggested it should be abandoned. Not long after that, it sunk without a trace,� Michael said.
They lived their lives well, and on their own terms.
Now their daughters waited on the beach. Their greatest fear was not that their beloved parents would die, but that they - or worse, one of them - would not. The Shaw sisters trusted their parents and had faith in their plan but they were still aware of the many things that could go wrong. What if the drug their mother had buried in her garden for fear of a police raid had lost its potency? What if one of them survived to be accused of killing the other?
Nobody knows precisely what happened in Peter and Pat�s last moments but when the sisters returned to the house, about 1.30pm, their mother was lying still on her back in bed. There was a note on the bench from their father in spidery handwriting. It said, in part: �Satisfactory for Pat and for me, eventually�.
They found their father in the shed, reclining in a chair. They checked for signs of life - or death. Heartbeat, pulse. First their mother. Then their father. Nothing.
VIDEO - not available at the moment - Anny Shaw discusses her parents, their deaths and the aftermath.
There is no good way to lose your parents. When the three sisters returned to their parents� house, they were orphans. The plan had worked and there was no sign of suffering. Peter and Pat had set out to end their lives in a meticulous, scientific fashion without any fuss, just as they had lived. And they had done it.
What happened next was unsettling, though. The sisters called their parents� GP. They had expected him to be able to come promptly and quietly certify their deaths.
But he was caught up with patients all afternoon. He told them the two deaths required a call to triple zero.
This was when the outside world started to push in. Within minutes of the call, paramedics arrived, lights flashing. The police were not far behind. Two people had died in a suicide pact and their three daughters were at their home. Suddenly, a very private decision had become a very public event.
Kate met the paramedics at the door. The medicos wanted to rush in. She stopped them to explain. Their parents had intended to die; they did not want to be resuscitated, she said. It took some discussion. Eventually the paramedics entered, attended the bodies and documented the deaths. They were respectful, say the daughters. The police were also sympathetic and supportive when they understood what had happened. But the homicide squad still had to be called in. The Shaw family home became a crime scene. The sisters were told to attend a police station to make statements. No charges have been laid.
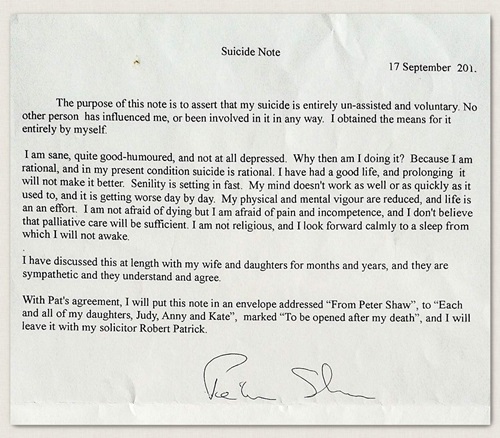
To erase any doubts about their deaths, Peter and Pat had both written suicide notes. Each said they had died by their own hand, with no assistance or pressure from others. In a letter left with his solicitor and titled �To be opened after my death�, Peter had written that he was �sane, quite good-humoured, and not at all depressed�. He said he was making a rational decision.
�I am not religious, and I look forward calmly to a sleep from which I will not wake,� he said.
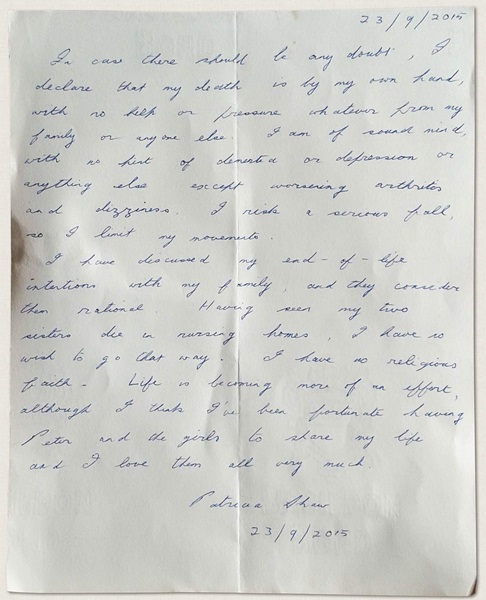
Pat wrote a note in her own cursive hand and tucked it into a notebook with the family�s �X�mas pud� recipe for her daughters. The note, written on cream paper, said she had no help from her family, whom she loved very much.
�I am of sound mind, with no hint of dementia or depression � Having seen my two sisters die in nursing homes, I have no wish to go that way,� the letter said.
Today the Shaw sisters are still coming to terms with the loss of both parents. They miss their wit and warmth. But they respect their choice and feel strongly that suicide can be rational. All three say their parents should not have had to risk prosecution to die together at the time of their choosing. Nor should they have had to be alone for the legal protection of their family.
�It shouldn't be so difficult for rational people to make this decision,� Kate said. �Obviously, care has to be taken but assisted suicide should not be illegal.�
Anny and Kate, the two sisters who have been willing to talk publicly about what happened that day, have been honest with many people about their parents� choice.
Some have been awed. Most have been deeply supportive. But a couple have passed judgement. One friend suggested Peter and Pat had been selfish for leaving their daughters. Another acquaintance hinted to the daughters that they must not have offered enough support. Why would their parents leave them if they knew they would be cared for?
But Kate says anyone who suggests this does not understand the Shaws, a family of fiercely independent rationalists. Her parents never wanted to leave their home nor be cared for. Nor were they the types to sit around for another decade with rugs on their knees.
�To those people who say we don�t have the right to choose the time and manner of our departure, our mother and father said, �Well, we do and we did�,� she said. �I love their defiance right to the end. But these were two extraordinary human beings.�
BELOW Peter and Pat on the day they died.
VIDEO - not available at the moment - Tom McKendrick PORTRAIT OF ANNY SHAW Joe Armao PRODUCTION/DESIGN Mark Stehle MULTIMEDIA EDITOR Felicity Lewis For help or information, call Lifeline 131 114 and beyondblue 1300 224 636
Article in The Age:
Thousands of older people are investigating peaceful methods to end their own lives because they want to control the nature and timing of their death, says controversial euthanasia campaigner Philip Nitschke.
The former doctor said there was a developing trend of baby boomers and people over 70 wanting to avoid "end of life medical nightmares" in which they are seriously ill and or feel trapped in a hospital or nursing home where it can be difficult to take your own life.

The head of Exit International said these people were "used to getting their own way and less likely to accept the 'doctor knows best' approach to issues as fundamental as one's death", and were sourcing a reliable lethal drug to stash in case they wanted to use it in the future.
Most of these people were putting themselves at legal risk to import and possess that drug, Mr Nitschke said, and some were getting caught up in blackmail scams where supposed suppliers threaten to report people to the police if they do not pay large sums of money online.
While customs are frequently intercepting the drug, Mr Nitschke said he knew of only three people in 10 years to be charged with importing it after customs tracked the order to them. All three received fines and were not convicted of a criminal offence.
Last week, Fairfax Media told the story of Peter and Pat Shaw � Exit members who took their own lives together in their home when they were both aged 87.
Before their deaths, they told their family they were rational, had lived full lives, and did not want to run the risk of further ill health and institutionalisation.
In response to their story, Mr Nitschke called for the decriminalisation of people aged over 70 who import or possess the drug he promotes for a peaceful death. He said while many doctors "peddle" a line that you cannot be rational and take your own life, he believed otherwise and that the Shaws were a good example.
Professor Ian Hickie, a psychiatrist and mental health campaigner, said he thought it was tragic that people wanted to "check out" of life because of myths and negative stereotypes about ageing, pain relief, hospitals and how the health system treats elderly people.
He said while some people may not have a mental illness when they end their own life, Exit International's approach to teaching people about suicide was reaching vulnerable people who could, with further assistance, live a longer, enjoyable life.
Professor Hickie, of the Brain and Mind Centre, said Australian authorities needed to work on policies and resources to promote healthy ageing with a focus on getting the right care and support to people so they do not feel like a burden and live as well as they can in their later years.
He said people considering suicide or families discussing the issue should examine what is underpinning people's motivation. Is it fear of being a burden? Is it fear of a lack of care?
"It's a dialogue we need to have � There shouldn't be a need to check out at any age."
For help or information, call Lifeline 131 114 or beyondblue 1300 224 636.Euthanasia letters in The Age:
I was deeply moved by Julia Medew's superb account of the lives and, eventually, self-managed deaths of Peter and Pat Shaw ("In death as in life", 16/1). May their story be the straw that breaks the logjam holding back the community's wish for legal assisted dying for those who find life no longer worth living. Yes, there need to be safeguards to protect the vulnerable or depressed. But it should not be so difficult as to require the degree of planning and ingenuity that the Shaws � both accomplished scientists � had to undertake. If this cause can be advanced by their action, it will be, perhaps, the crowning contribution from their remarkable and inspiring lives.
Michael Hassett, BlackburnOne can only admire the actions of Pat and Peter Shaw in ending their own lives in their own way. Few would have the courage. There was, however, one highly upsetting aspect to this uplifting story. It was that their daughters could not be with them at the end, for fear of prosecution. Even if assisted suicide remains illegal, could not legislation be enacted that allows one to create a living will to exclude specific named people from the threat of prosecution? Explicitly, I don't want my children to be charged with my murder ... ever.
Bill Jacobs, Mount WaverleyThe Shaws had a "sense of a life accomplished", happy and content. They were aware, however, of the cruel hand that death could deal to those in their latter years and tarnish what had been lifetimes of achievement and fulfilment. They realistically accepted death as imminent and deemed their future quality of life to be unbearable. They were not afraid of death but feared the manner of their demise. Between them they made a competent and selfless decision to end their lives at a time of their own choosing. Their courage and that of their three children was remarkable. What a sad indictment on our society that such wonderful people were forced to manage their own deaths covertly. Suffering in death is indiscriminate but for those who succumb, it can be cruel and torturous and may leave loved ones scarred and fearful of death. We are granted the right to make so many life choices, why not in death too?
Jane Morris, MalvernThank you for the fine report on Pat and Peter Shaw. The online presentation is exquisitely designed and I'm sure will be treasured by their daughters. If all of us could bear to consider how we'd like to die, I reckon most would want to go like the Shaws. But it's easier to push the thought away. And even the non-religious seem somehow to believe that dying is the ultimate harm, to be delayed in any circumstances. Surely our society needs to reassess its attitudes to death and dying as more of the ailing elderly are crammed unwillingly into inadequate hostels and nursing homes. This is not a call for involuntary euthanasia, simply a request for sympathetic assistance to those who rationally want to take their leave when continued living would be worse to them than death.
Anne Riddell, Mount MarthaPat and Peter Shaw have shown that sane, rational, intelligent people can, with a bit of luck, stay out of the clutches of the slow-death industry of palliative care and excessive medical intervention and have a dignified death at a time of their choosing, with a loving farewell from the family.
Kishor Dabke, Mount WaverleyProfessor Ian Hickie refers to those "of later years" as being vulnerable, gullible to those preaching negative stereotypes as though voluntary euthanasia were the latest flavour of the month ("Increase in elderly considering suicide", 18/1). While it is worthwhile to work on promoting healthy ageing, no one can make an accurate, objective assessment of whether another person's life is enjoyable or satisfying to them � not even a psychiatrist.
Beverley McIntyre, CamberwellI read the account of the self-managed deaths of the Shaws and the following letters with unease. My husband died when I was 72 and life no longer had any meaning for me. I desperately wished to join him in death, and had the means been available would have done so. For about six months. Then I began to feel better. Two years after his death I fell happily in love again. Now, 11 years after his death, although I still miss my husband, I can say life is very good. Thank goodness I did not have the means to end it when I wanted to.
It is horrible to think of life being extended into an unbearably painful and undignified old age. If that should happen, one would hope for a kindly, courageous doctor who would realise when enough is enough and ease one's parting. But making the means available to end one's life at a time of one's choosing involves more issues than have been debated.
Judith Wallace, HarkawayIt is high time the community was rid of the fear of prosecution if they are present when loved ones end their lives as Peter and Pat Shaw did. Victorian criminal law states it is an offence to "aid and abet suicide". This means one has to do something, to be practically involved. Just being present to say goodbye is not a crime. No one has ever been prosecuted for simply being present. Following a two-year investigation into the death of Nancy Crick, at which 21 people were present, the Queensland Police Commissioner stated that "being present when someone takes their own life does not constitute an offence". If the death is reported to the coroner, the police will interview anyone known to be present, but this is a formality to provide the coroner with information, and not for the purpose of prosecution.
This widespread ill-informed view condemns many people to die alone. This could easily be corrected if the Office of Public Prosecutions issued a statement to clarify the matter.
Dr Rodney Syme, ToorakThe Shaws' GP was wrong to tell the family to call triple 0, but I can understand his reluctance to get too involved. When the wonderful Beverly Broadbent told me she was planning to kill herself, nearly three years ago, I agreed to write her death certificate. I had always known of her intentions, and as her GP of 15 years I was prepared to respect the last request of this remarkable woman. The result was 2 years of legal uncertainty while the Medical Board and the coroner investigated my actions. The laws around voluntary euthanasia must change to provide clarity for all those involved.
Dr Nick Carr, St Kilda
It is tragic that older people commit suicide (The Age, 17/1). The National Coronial Inquiry Service estimates that two people over the age of 80 are taking their lives every week. The most common method is hanging.
Ian Hickie suggests older people commit suicide because of myths and negative stereotypes about ageing, pain relief, hospitals and how the health system treats elderly people. Are these myths? Recently, an elderly woman living in an aged care home died in excruciating pain because no one was suitably qualified on the night shift to administer the prescribed morphine. The woman's daughter was so traumatised she could not remain at her mother's bedside to hold her hand.
We do not need motherhood statements about healthy ageing. We need political action to ensure older Australians are valued and receive the quality of health care that they deserve.
Sarah Russell, NorthcoteMany years ago, funding to aged care facilities was allocated and monitored according to how it was used � for care, general services or administration. Not now. Governments require facilities to regularly undergo an approval process to prove they are providing services of the required standard to maintain funding. This means facilities employ expensive consultants to provide this evidence for the period of assessment. Those of us who regularly visit these facilities know all too well when an assessment is imminent as processes are visibly ramped up for assessment, only to be wound down after approval for the coming years is granted. We must return to a system where money for care is quarantined from that used on administration.
Jenny Callaghan, HawthornArticle in The Age responding to Pat and Peter Shaw euthanasia article above:
When my article about Peter and Pat Shaw, the husband and wife who took their own lives, went up on Fairfax websites at noon last Friday, I didn't know what to expect.
Would our readers click on a story about an elderly couple's suicide pact? Or was it too much for a sunny afternoon at the end of the week?
Within an hour of publishing "The Big Sleep" online hundreds of people were reading the story; an encouraging start, if not out of the ordinary.
But by the next morning, by the time the story had then appeared in print, something had changed.
On my personal Facebook page, people of all ages were sharing the article, urging friends and family to read it. Then the emails, phone calls and text messages started.
Parents of children I'd gone to school with; cousins; colleagues; CEOs, politicians; doctors; people I had not seen for years. They all felt a compulsion to talk about it. They clearly felt that Peter and Pat Shaw, who had decided to end their lives before their bodies and minds deteriorated further, had done well to avoid that suffering. One old friend wrote to say that her father had flagged his intention to take his own life one day in the future and that she felt deeply conflicted about it. The Shaws' story had made it easier for her family to discuss it.
Doctors and social workers who work in aged care emailed to say that they were saddened by the lack of choice around death in Australia. One emergency doctor said she had cared for elderly people who wanted to die while their families demanded "everything" be done to keep them alive. "Sometimes they scream they want to die, or that they don't want me to touch them," she said. "I then have to decide how far I need to go with treating the patient."
We estimate the story has now been read by nearly a million Australians. Thousands have made the effort to comment on the Facebook posts about the story, many sharing their own, often harrowing, experiences of seeing loved ones die in difficult circumstances.
"My father died a horrible death in an aged care house," wrote Trianta Karalis. "My mother is slowly going mad from dementia." Rhonda Purcell wrote of her mother's "living nightmare" with dementia in a nursing home. Cushla Wise recalled her mother's "long, slow, undignified death with Parkinson's and Lewy body disease".
Gillian McAlpine shared that her mother "spent the last six years of her life in a long-term hospital setting, confused and lonely". Michael Finn told of his parents' last months, and wondered "if this would have been different if they'd had the option (of suicide)".
Donna Close told us: "I don't want to see my parents suffer. I want to remember them as bright buttons who filled our hearts with love."
There were hundreds more in a similar vein.
Not everybody agreed that the Shaws' story should have been told. One person on Facebook accused The Age of glamorising suicide; another tweeted that it would encourage people to take their own lives.
One man with a history of depression wrote to say it was irresponsible journalism and that people would certainly die as a result. "Knowing how suicidal people think, I can guarantee your articles have and will lead to people in this frame of mind� taking their own lives," he wrote.
We were mindful of this before the story was published. In an effort to minimise the risk for vulnerable people, we decided not to detail the methods that Peter and Pat used. We also included help lines for people to call if they were troubled by the story.
Keryn Curtis, a journalist who writes about ageing, noted that "dignified", "respect" and "choice" were words that recur in the comments about the article. "As an observer of this topic over the last decade or so, it feels to me as though the tide is really on the turn," she wrote on the website, Frank & Earnest.
"What seems to have changed is not so much the number of people who would like the choice of an assisted death (although that may be changing too) but a couple of other things: one, an increased willingness to speak out publicly in great numbers; and two, an emerging willingness on the part of those who would never personally make that choice, to accept the right of others in certain circumstances to have that choice."
The Shaws' story resonated for a reason. It highlighted an uncomfortable truth; that many Australians value their quality of life and do not want to live beyond a certain point that might be intolerable to them. Their voices are getting louder.
Euthanasia letter in The Saturday Age:
Jennifer Philip presents a lovely scenario of dying with dignity (Comment, 22/1). But she misses the main complexity that worries us oldies. We're not really concerned about "unbearable suffering". We embrace the realities of palliative care.
What we are concerned about is dementia; being kept alive (without machines) for years while being mentally missing.
Until doctors or friends are allowed with our express permission to put our bodies where our minds have already gone, we must plan and execute our suicide well before we become demented. Otherwise we risk becoming what we � and, in all honesty, our friends and family � would abhor: a pointless drain on everyone.
Wouldn't Jennifer Philips' scenario be different in that case?
But getting that timing right is a really hard call, so I'd rather spell it out in my advance care plan, and have my doctor do what vets routinely do to pets that are as much loved as any person.
Peter Greig, MurroonEuthanasia letter in The Age:
When I received a diagnosis of multiple sclerosis in December 2014, I was frightened. Death did not scare me, but the prospect of disability did. So I found out all about the disease and available treatment. I also investigated methods of euthanasia. By undertaking the latter, my feelings of fear were reduced. Hopefully, I will never need to go down that route, but am comforted that the option is there. It's not my place to impose my views/values about euthanasia on others and I therefore do not expect others to try to impose their dogma on me.
Susan Nisbet, Caulfield NorthArticle in The Age:

The Victorian Parliament's upper house committee of inquiry into "End of Life Choices" has produced a remarkably comprehensive and erudite report. The public and institutional response to the inquiry has been greater than for any previous inquiry. There were 925 individual submissions and 112 from organisations. In addition, the majority of committee members took the trouble to visit countries where jurisdiction allowed some form of assisted dying. Notably, the dissenting members of the committee did not avail themselves of this information and first-hand experience.
Quite rightly, the committee focused on empirical evidence and scholarly research rather than personal opinion. Nevertheless it did not disregard the latter and noted that these submissions, like reliable evidence of public opinion, overwhelmingly supported legislative reform. Numerous submissions detailed tragic deaths, some occurring in palliative care. The submissions, particularly of the Coroner, Victoria Police and the Australian Nurses Federation made an obvious impression. The factual data gained from visits to the Netherlands, Switzerland, Canada and Oregon allowed the committee to study different approaches to assisted dying legislation, and to be assured that these legal frameworks worked well in practice without evidence of abuse.
The most important voices raised against legislative change, as the inquiry noted, came from the Australian Christian Lobby, the Catholic Archdiocese of Melbourne, the Australian Catholic Bishops Conference, the Australian Family Association and Doctors Against Voluntary Euthanasia. And, notably, Palliative Care Australia. The Australia and New Zealand Society of Palliative Medicine has about 400 members, a small fraction of Australasia's medical community, yet it seeks to determine government policy on voluntary assisted dying. Some 85 per cent of its members oppose assisted dying, in marked contradistinction to the public, the people it is supposed to serve.
This brings me to the views expressed in The Age (June 21) by Professor Peter Hudson, who made a number of criticisms of the report. I hope his article leads people to actually read the report (especially chapter eight). The report does not recommend legalising "euthanasia and assisted suicide". The report recommends the government develop legislation for a bill for "assisted dying" � it does not use the pejorative word "suicide" in this context because it is inappropriate. It recommends that a doctor, under specific conditions, be able to prescribe lethal medication for his or her patient to self-administer � this is not euthanasia (lethal injection). However the committee recognised that very occasionally there may be people with enduring and intolerable suffering who cannot self-administer (who cannot swallow, or are completely paralysed). These people should not be discriminated against, and in this rare circumstance (I have never come across it in 25 years of counselling), and only this circumstance, a doctor could administer, because of necessity, a lethal injection.
Professor Hudson argues that "a controlled peaceful pain-free death cannot be guaranteed" by voluntary assisted dying because "people respond differently to these drugs (sometimes unfavourably) and the time taken to death will vary". How would he know? Palliative care does not use such drugs, and I will wager he has never been present when an assisted dying has occurred. I can vouch for the fact that, with appropriate preparation, the correct dose of Nembutal will reliably result in a peaceful sleep in three to five minutes with an assured death in 15 to 20 minutes. Can palliative care give the same assurance about terminal sedation? No � it is a process which can take five to seven days.
Even more extravagantly, Professor Hudson states that the committee advocates the untried Quebec legislative model. This is false � the committee considered a number of successful overseas models, and determined to recommend a model which was consistent with Victorian values. This model was not based on an untried model but on frameworks in use in Oregon (for nearly 20 years), the Netherlands (for over 30 years) and Switzerland (for more than 60 years).
Hudson states that "dying at home is not the gold standard or the only treatment option". Although their own home is where over 70 per cent of Victorians wish to die, only 15 per cent do so, largely because of the protracted nature of dying today. There is nothing in the recommendations of the committee that dictates where people must die.
Professor Hudson suggests that "the overwhelming majority of Victorians living with terminal illness who elect to receive usual end of life care rather than assisted dying will be receiving less health professional support under the proposed model". He bases this on two worthwhile but relatively minor recommendations in the report � first, that persons requesting assisted dying may be "allocated a specially trained nurse as a careworker", and secondly, that "healthcare professionals involved in providing euthanasia/assisted suicide will also be offered counselling". This is nonsense. Far more people in Victoria receive palliative care (with its on-call specially trained nurses) than would ever make a request for assisted dying, and secondly Professor Hudson should be acutely aware of the "burnout" of palliative careworkers faced with the inadequately relieved suffering of patients in their care. They need counselling too, and I hope they get it. Without doubt, this end of life work is difficult, however it is managed.
As the committee makes clear, end of life care should be patient-directed, with the suffering person making decisions based on their values and their own assessment of their suffering � not the assessment of a palliative care doctor who is adamantly opposed to what is an effective, humane, peaceful and dignified end to that suffering.
Dr Rodney Syme is a medical specialist who over a long period has given many terminally ill people the means and knowledge to end their life.
Article in The Age:
Aristea loves her grandmother dearly. Much of her childhood has been spent at her the Northcote home of her 'yiayia', eating stuffed tomatoes and cheese cake, doing homework and trading secrets in Greek.
Courageous girl's euthanasia speech for PM"Now is the time to make the change," 12-year-old Aristea told the prime minister. So she wrote him a letter.
So it took enormous strength for the 12-year-old to fight for her yiayia's right to die.
"If she wants to end her pain, I think that's her choice."
12-year-old Aristea is fighting for her ill grandmother's right to die. Photo: Pat ScalaAristea's grandmother has told her family she no longer wants to endure the severe, relentless pain of untreatable osteoarthritis. She feels anxious about the next time her pain will become unbearable, and says wants the option to put a stop to it.
"At first, I felt a bit sad. I thought, she wants to kill herself," Aristea tells Fairfax Media.
But the grade six student has grown increasingly distressed by her grandmother's deteriorating condition. She decided she had to act.
So she wrote to Prime Minister Malcolm Turnbull, demanding he change the law.
In a strongly worded three-page letter, she argues that terminally ill Australians were resorting to "repulsive", inhumane methods to kill themselves.
She compared the situation of a terminally ill Australian patient, forced to consider starving themself to death, with that of a "cancer victim in Luxembourg [who] rests peacefully in his hospital bed, holding his family's hands and ending his life harmoniously," she said.
"It is utterly appalling how extremely ill patients are required to put themselves through more unnecessary pain. How can people allow this?"
"Like the yin and yang or two sides of a coin, human life cannot occur without death.
"Consequently, those who argue that every human has the fundamental right to live, unknowingly also consent to the fact that every human has the rudimentary right to die."
Aristea also argued that people should have the right to a life of quality, rather than quantity "by allowing people to determine the how and when of their death, we are guaranteeing they will live what remaining life they have to the fullest; free from the pain of anxiety."
12-year-old Aristea with her grandmother Voula. Photo: Pat Scala
Her grandmother, Voula, showers her with life lessons: study hard, enjoy life while you're young, and fight for what you believe.
The 79-year-old grandmother is growing weak, becoming bedridden for weeks at a time. She is responding poorly to medication and unfit to have surgery.
The grade six student wrote to the PM about the issue as part of a project at Clifton Hill Primary School.
"Euthanasia is currently in favour of the country, and has been since 1964. Not respecting these wishes that your citizens hold will no doubt, in their eyes, demote you," she wrote.
Aristea points out that euthanasia is legal in the Netherlands, Switzerland, Belgium, Luxembourg and some US states.
A recent Victorian parliamentary report recommended the state government legalise assisted dying for people suffering from serious terminal conditions.
But Mr Turnbull has indicated he does not support euthanasia, while Labor and the Greens have said they would allow their members a free vote. Aristea, who also sent her letter to Premier Daniel Andrews, said the Prime Minister still owes her a response to another letter she sent him, in which she suggested changes to the design of wind turbines.
(She has also interviewed Alex Bhathal about "active citizenship" earlier this year, in between playing piano, the cello, and writing a crime story.)
"If he [Mr Turnbull] doesn't respond it's like he is avoiding it. And, I took a lot of time on it, so I think that he should be able to notice that and take some time to reply � I hope he will."
Read the full letter here: timna.jacks@fairfaxmedia.com.au
Article in The Age:
� September 13 2016 The AgeVictorians may be able to access voluntary euthanasia in the near future, after Health Minister Jill Hennessy declared she supports it and that the parliament and Labor government had to look at the issue closely.
Earlier this year a cross-party parliamentary inquiry recommended Victoria introduce voluntary euthanasia.
Euthanasia around the worldAdvocate Andrew Denton on Australia's crucial role in spreading euthanasia laws around the globe.
As Health Minister, Ms Hennessy is responsible for the Andrews government's response to the inquiry, which is due by December
"I believe that as a government, and as a parliament we need to look at euthanasia very closely," Ms Hennessy told Fairfax Media.
Photo: Jason South"Personally � and I believe personal experience plays a strong role in informing people's views on this issue � I support euthanasia."
"I also think it is clear community sentiment has shifted on this issue, and there is significant community debate around euthanasia at the moment.
She said as responsible minister she was carefully examining all of the committee's work and that if Labor did pursue euthanasia proper safeguards would be put in place.
On Tuesday the Andrews government introduced new laws to parliament to make advanced care directives legally enforceable.
Victorian Minister for Health Jill Hennessy. Photo: Darrian Traynor
In the strongest indication yet that Labor may introduce laws to allow euthanasia, Ms Hennessy did not rule out a scheme when pressed on Tuesday, saying the inquiry had widely canvassed community views and that of the medical and a legal professions.
"I don't have a religious or ethical objection to euthanasia," Ms Hennessy said.
"There are great opportunities for us to provide a better death for Victorians."
She said the inquiry's recommendation around an assisted death scheme was something she had "a very open mind" towards, but the decision was ultimately for the whole government.
"I think the material canvassed in the inquiry is very good."
Labor introduced new laws on Tuesday to parliament to make advanced care plans legally binding.
The directives currently give patients the power to set certain terms and guidelines for their doctor at the end of life but are not enforceable.
The new laws will make it clear for health professionals what a patient's preferences are, and for the first time in Victoria make breaching these preferences a matter of misconduct, with deregistration a possibility.
The bill states that patients cannot reject palliative care because of clinical feedback that not all people understand what pain and death is actually like, Ms Hennessy said.
The law will apply, with rigorous checks and balances, to children as well.
"We've put some carrots and sticks in the bill," she said.
The conversation people have around their death needs to become more culturally acceptable, with Ms Hennessy calling on more Victorians to talk with their GPs about death.
"We want to change the culture around people not having these conversations around a barbecue or a dinner party table. We want them to happen with their GPs and clinicians and to commit an advanced care plan to writing," Ms Hennessy said.
There will also be safeguards around a person's level of mental capacity in making an advanced care directive, with power of attorney laws.
The minister said there was not enough policy focus on the end of life.
"Our historic new laws will give Victorians the certainty they want and need when it comes to end-of-life care and wishes," Ms Hennessy said. "We're putting people's preferences and values first when it comes to medical treatment decision making."
Dying with Dignity Victoria welcomed the fulfilment of Labor's election commitment.
"This and changes to palliative care services to meet community expectations represent a significant step forward," said Lesley Vick, DWDV president.
"The framework recognises that current practices do not meet community expectations, notably that many people wish to die at home but are unable to do so," she said.
Any euthanasia laws would be subject to a conscience vote on both sides of politics.
Greens MP Colleen Hartland said the government needed to introduce euthanasia laws as soon as possible and if the government failed to do so, the party would introduce a private member's bill.
"There is overwhelming support for assisted dying to be made legal. The government needs to step up to the mark and give terminally sick people the power to end their suffering," Ms Hartland said.
"We welcome people being given control over medical decisions through advance care plans, but want terminally sick people to also be given the choice to end their lives."
LINKS
Red Jos: HUMAN RIGHTS ACTIVISM
Mannie and Kendall Present: LESBIAN AND GAY SOLIDARITY ACTIVISMS
Mannie's weblogs may be accessed directly by clicking on to the following links
Activist Kicks Backs - Blognow archive re-housed - 2005-2009
RED JOS BLOGSPOT (From January 2009 onwards)
This page created on 20 MAY 2015 and updated on 10 MAY 2018
PAGE 87